Top News

Microsoft extends its Dragon Copilot AI clinical assistant to nurses and adds an ecosystem for third-party extensions.
The nurse capabilities include ambient documentation, access to trusted medical content, and automating routine tasks.
Reader Comments
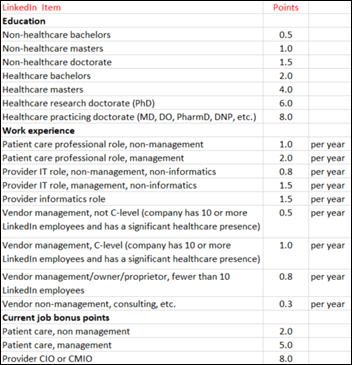
From Boysenberry: “Re: self-proclaimed industry experts. You proposed a scoring framework years ago that took into account clinical and IT experience from someone’s LinkedIn profile. Where is that?” I remember it, but I can’t find it despite many searches via Google and ChatGPT. I do recall that some of the folks who were dispensing unsolicited health tech advice scored low, having little actual experience other than in pontification. UPDATE: found it from 2017! See scoring grid above. I didn’t do much with it, and the low-scoring folks are still out there pontificating, so the effect was minimal. In fact, the vastly lowered barrier to entry for podcasts has probably given a whole new batch of industry lightweights a place to hear themselves talk.
From New Threads: “Re: corporate rebranding. Why do companies think anyone cares about why they chose a particular logo or website design?” I assume these “our redesigned website shows how we’ve evolved” posts exist mostly so the marketing folks who justified the project can get their ceremonial pat on the head. There’s always a tortured back story that someone has wasted time inventing about how the lowercase typeface represents empathy and the color gradient evokes innovation, when in reality, nobody outside the company cares. Announcing it just makes everyone else uncomfortable, like bragging about how great you look in your new suit while everyone’s politely trying not to roll their eyes because they are perfectly capable of forming an opinion without an announcement or editorializing. They also know that appearances aside, it’s still the same person underneath.
A Reader’s Notes from Global Health Innovators Summit, Nashville

Investment panel
Vic Gatto, Jumpstart Health Investors
- He says AI will cause a four orders of magnitude (10,000x) change to what we can deliver in healthcare.
- Current AI investments focus on workforce; he thinks we’ll need just as many people in healthcare despite AI.
- He sees a barbell of success for healthcare investing. On one end are solutions that cater to wealthy individuals, like biometrics and whole-body scans. On the other end are solutions that touch the low-income side of the market (e.g., Medicaid) and squeeze out efficiency gains and cost savings.
Tania Grant, Partner, Claritas Capital
- AI valuations are overhyped and expectations will have to come back down to earth at some point.
Fireside chat with Chris McGhee, CEO and Co-Founder, Current Health
- He thinks it’s a very difficult time to build a digital health company, partly because of inflated capital raises and inflated valuations that many companies can’t keep up with.
- The hardest part of the acquisition by Best Buy was the culture change and the difficulties integrating into a totally different culture. Incentives and pace of change are radically different at a big public company.
- When he reacquired Current, it had three times the number of employees as when he sold it. Had to let go about 100 people from the get-go, and he noticed that the culture had lost the customer focus and urgency.
- They’re focused on CAR-T therapy and moving that to the outpatient setting.
Panel on data utilities, policy, and regulation
Brenton Hill, Head of Operations and General Counsel, Coalition for Health AI
- CHAI views transparency as table stakes and has been placing a greater emphasis on transparency.
- A key thing to figure out is who is responsible for an AI solution over the course of its life cycle. Is it the developer or the health system/payer who has deployed it?
- The current regulatory framework for healthcare data is not built for AI. AI moves at the pace of governance, not government. He says we should look at governance not as an inhibitor but as what will allow AI to scale.
Brett Meeks, Vice President of Government Affairs for Health Technology and AI, Kimbell & Associates
- Government is struggling to regulate technology, given the fast pace of change.
- He expects the current administration to follow through on enforcing info blocking regulations.
- He floated the idea of states using the $50 billion rural health fund from the OBBB Act to incentivize EHR adoption in behavioral health.
Peter Embi, Department of Biomedical Informatics, Vanderbilt University Medical Center
- VUMC has built a tool that monitors the 200+ AI systems they are using throughout the health system. The tool checks for algorithm drift and impact on health equity.
Panel on innovation in cancer care
Lauren Connor, breast reconstructive surgeon, Vanderbilt University Medical Center
- A key advancement in treatment and reconstruction in breast cancer care has been minimally invasive procedures, and those have been made possible by robotics.
Jillian Wright, CEO, Onsite Women’s Health
- They’ve seen screening mammogram compliance rates go from 50% to 85% when the mammograms are offered in-clinic by primary care providers.
Abbey Vandersall, Chief Clinical Officer, AMSURG
- Any solution that boosts compliance is a value-add. Only 50% of patients who use Cologuard and get a positive result actually follow through with the necessary confirmatory colonoscopy.
Sponsored Events and Resources
None scheduled soon. Contact Lorre to have your resource listed.
Acquisitions, Funding, Business, and Stock
MD Integrations, which offers a white labeled telehealth service to digital health companies, raises a $77 million investment.

Senior platform vendor Cairns Health acquires Together by Renee, which offers a personal healthcare assistant.

Remote care company Brook.ai raises $28 million in Series B funding.
Sales
- UPMC will extend its deployment of the ambient documentation solution of Abridge, in which it is an investor and founding site, to all of its locations.
People

Harmony Healthcare IT hires Sharon Cook (Inovalon) as chief revenue officer.
Announcements and Implementations
Redox and Kno2 partner to offer unified integration, data translation, and nationwide TEFCA connectivity.
Mount Sinai researchers develop InfEHR, which scours a patient’s EHR lab results, medications, and vital signs over time to create a personalized network that discovers hidden associations with disease state.
Altera Digital Health announces GA of Sunrise Axon, which was built in partnership with Health Gorilla to bring real-time clinical data into Sunrise EHR.
Wolters Kluwer Health releases UpToDate Connect, which offers developers API access to its evidence-based clinical content.
Surescripts introduces First-Fill Abandonment, which alerts care managers when patients fail to have a first-time prescription filled.

Lapsi Health launches Keikku 2.0, a $375 FDA-cleared digital stethoscope that uses AI to generate clinical notes that are integrated into the EHR.
Digital health marketplace operator Avia acquires Panda Health, which offers digital health peer input and market intelligence services.
Government and Politics

HHS’s new Medicare Plan Finder provider directory, which was built by a vendor under the administration’s “Make Health Tech Great Again” program, is generating conflicting or inaccurate listings about whether providers are in-network for Medicare Advantage plans. The tool also limits searches to providers within 50 miles and excludes hospitals and skilled nursing facilities. Errors in the temporary open enrollment site, which was intended as a first step toward a national provider directory, could mislead seniors into choosing plans that their doctors don’t accept. A previous CMS announcement suggests that the directory’s developer is SunFire Matrix, a private equity-owned services platform vendor that sells similar tools to insurance brokers.
Privacy and Security
Integris Health pays $30 million to settle a class action lawsuit related to a 2023 data breach that impacted 2 million people.
Other
In England, NHS administrator Sir Jim Mackey requires NHS England’s transformation directorate to personally sign off on readiness before electronic medical records are brought live during the busy winter period.

Keep scrolling if health tech history isn’t your thing (or if it is, go deep with Vince Ciotti’s magnificient HIS-tory). Industry veterans will appreciate John Gomez’s insider recap of what onetime frontrunner Eclipsys got wrong during his time as CTO (spoiler: dismissing Epic as being too small to threaten Sunrise Clinical Manager). He generously avoids blaming the unremarkable Eclipsys CEOs who followed founder and industry legend Harvey Wilson through the early 2000s, namely Paul Ruflin and Andy Eckert, neither of whom had recent relevant experience (they must have learned hard lessons since they’ve done fine since in other health tech leadership positions). Then came Phil Pead, who had the savvy to sell publicly traded Eclipsys to Allscripts for $1.2 billion in 2010, only to be fired in 2012 in a power struggle with Glen Tullman. Allscripts was a slow motion car crash under Tullman, but maybe it wasn’t his fault (ever-stumbling Misys was its majority owner) since after the company fired him, he became health tech investing’s golden boy by launching 7wireVentures and unloading Livongo on Teladoc for $18.5 billion in 2020.
Sponsor Updates
- Altera Digital Health publishes a new client story titled “On the way to the peak: Scaling technology at Wyckoff Heights Medical Center.”
- Judi Health releases a new episode of “The Astonishing Healthcare Podcast” titled “Addressing Barriers to Drug Access & Affordability, with Valeris’ Andy Glade.”
- Agfa HealthCare powers enterprise imaging modernization across North America.
- Wolters Kluwer Health and Vanderbilt University’s Heard Libraries collaborate on a transformative medical research agreement.
- Ellkay will exhibit at NextGen Healthcare’s User Group Meeting November 2-5 in Nashville.
- Fortified Health Security announces that it has been named the winner of the “Managed Security Innovation of the Year” award in the CyberSecurity Breakthrough Awards.
- Healthcare Growth Partners publishes “Observations – October 2025.”
- Black Book Research founder and CEO Doug Brown will deliver the keynote address at OpenEHR’s EHRCON25 conference.
- Health Data Movers names Joshua Arkin account manager.
- Impact Advisors publishes an analysis of the One Big Beautiful Bill Act and the economic effects it may have on providers.
- Inbox Health exhibits at the American Medical Billing Association National Medical Billing and Coding Conference through October 17 in Las Vegas.
- Aspen Medical will implement Meditech Expanse at its two hospitals in Fiji.
Blog Posts
Sponsor Spotlight

Findhelp is powering a more connected and efficient social safety net. They’re replacing fragmented systems with a modern, digital infrastructure that streamlines social care delivery from start to finish, from identifying needs and authorizing services to tracking data and ensuring better outcomes. Findhelp’s solutions support the entire care journey, including state benefit eligibility workflows to drive successful redetermination and post-acute care and behavioral health networks to provide whole-person care. They now work with 157 payers, 217 hospitals and health systems, and 88 health centers (and growing). Connect with Findhelp on LinkedIn to stay up to date on their work. (Sponsor Spotlight is free for HIStalk Platinum sponsors).
Contacts
Mr. H, Lorre, Jenn, Dr. Jayne.
Get HIStalk updates.
Send news or rumors.
Follow on X, Bluesky, and LinkedIn.
Sponsorship information.
Contact us.































Re: A chief health AI transformation officer (CHAITO) I predict a position evolution along the following lines. "We have too…