EClinicalWorks will pay $155 million to settle a federal False Claims lawsuit alleging that ECW misrepresented its EHR product and paid customers kickbacks for promoting it, the Department of Justice announced today.
The government claims that ECW fraudulently obtained certification for its EHR by hard coding some of the testing elements as provided to its certifying entity. It also says ECW’s software did not accurately maintain a user audit log, did not reliably record diagnostic imaging orders, failed to perform drug interaction checks, and failed to meet interoperability requirements, thus causing false claims for HITECH incentive payments to be paid by HHS.
According to ONC’s Certified Health IT Product List, ECW’s Authorized Certification Body is Drummond Group.
The company and three of its founders will pay the $155 million settlement.
ECW also entered into a five-year HHS OIG Corporate Integrity Agreement that requires the company to have its software quality control systems externally audited and reported to HHS OIG. The company also agreed to provide prompt notice to customers of any EHR-related safety issues, to make software updates available at no cost, and to assist customers in migrating to other EHRs without charging them. ECW is also required to hire an Independent Review Organization to certify that the company’s agreements with providers comply with anti-kickback laws.
The whistleblower lawsuit was filed by Brendan Delaney, a software technician with New York City Division of Health Care Access and Improvement, who will receive $30 million of the settlement.
I’ve run several reader-provided rumors about the Department of Justice investigation, going all the way back to late 2015.
An internal UCSF study finds that 82 percent of the text in a typical Epic progress note comes from copying/pasting or importing from other sources. Clinicians physically enter only 18 percent of the note.
Several hundred of the 24,000 notes reviewed contained no human-entered text at all.
The study is especially interesting because it used a new text analysis tool – apparently provided by Epic – to determine the source of every character of text in the note.
Reader Comments
From Jack Fruit: “Re: CommonWell. Who were the original members?” CommonWell Health Alliance was founded in March 2013 by Cerner, McKesson, Athenahealth, Greenway, and RelayHealth (which is also owned by McKesson) as the Epic fears of the publicly traded competitors intensified to the point that they cooperated (and pony up a rumored $2 million each) to have something to announce at HIMSS13. Since then, McKesson has mostly pulled out of healthcare IT by spinning off Change Healthcare and looking for a buyer for its enterprise business and Greenway Medical Technologies was taken private by Vista Equity Partners a few months after the CommonWell announcement. Athenahealth shares are up 38 percent since the announcement, those of Allscripts are down 10 percent, and Cerner shares have risen 41 percent as all the founding companies have tried to diversify themselves out of a HITECH-free EHR market. CommonWell later added CPSI (now Evident) and Sunquest as founding members in mid-2013, but Sunquest is no longer listed as such on its site even though Sunquest’s site still says it’s a member.
From Kathy: “Re: CommonWell survey. It would be most accurate for me to vote that it performed exactly as I expected – which was very little. CommonWell was never going to work. It was a political and business tactic.” Above are the early poll results.
From Tammy: “Re: CommonWell. I work for RelayHealth supporting the CommonWell network. CommonWell is not one EHR, it’s a network. It brings together multiple health IT systems and helps to solve the challenge of connecting disparate software run by different companies, using different technology. People’s definitions of numbers are different depending on what and how they count. What really is important is that we are all working towards helping providers and people get access to important health data that they previously couldn’t. CommonWell is definitely moving the meter in the right direction on this. What is different about what CommonWell is doing is that providers don’t have to search for records and guess where they might be located. They also don’t have to download and store every document for their patients – we’re about making it more efficient to get the data that is most valuable to the provider when they need it. Providers can query and view what documents are available, similar to a search engine, and only download those they need. I have seen 2x the volume of query and retrieval growth in the past year.”
From David McCallie (Cerner): “Re: CommonWell. It seems like a case of apples to oranges – it would be bad math to compare numbers that aren’t measuring the same thing. For Cerner, CommonWell queries are a small (but important) fraction of Cerner’s overall document exchange interoperability. We don’t know exactly what counts as a ‘record’ or gets included in Epic’s CareEverywhere statistics, but for Cerner, document exchange includes not only CommonWell, but also many existing point-to-point query interfaces (via Cerner Resonance, including many connections to Epic clients) as well as local HIE-based document queries, and data routed to providers through the ‘Cerner Hub’ services. Cerner also supports a growing Direct-based document exchange. To the clinician, these are all equally available sources for external documents and data. In general, the user interface does not distinguish the means of transport. CommonWell in many ways represents a national-scale ‘back stop’ for data that can’t be found via local queries. Now that CommonWell and Carequality have committed to mutual interchange, we expect that the number of CommonWell-mediated transactions will grow, since CommonWell will provide a common gateway to both its own network as well as any requested Carequality sites. CommonWell automatically bundles an MPI and a national Record Locator Service, so the clinician does not need to spend time deciding where to look for documents that aren’t local. Don’t count CW out … the network is growing, and any numbers they report represent a very high quality of interoperability use case.”
From Spiker: “Re: health IT writing. Biggest problem is advertiser-friendly puffery. And mistakes like this one.” I disagree. The biggest problem is writer naiveté even in the absence of advertiser bias (unintentional or otherwise). Gushy, “world peace” kinds of health IT articles are always written by folks who have never actually worked in a health IT or clinical leadership role and thus have not learned from hard-won experience to distrust vendors, politicians, and health system executives until they provide a reason to believe otherwise. They’re also scared of being called out for lack of knowledge, so their writings tend to be harmless little bubbles floating aimlessly above the fierce, patient-impacting HIT battles being fought. The bar I set for everything I read regularly (especially if it expresses editorial opinion) is:
Does the writer enough knowledge and experience to be trusted?
Does the article tell me something I didn’t already know?
Can I really use the information?
Does the writer present the information clearly, concisely, and at my level, without time-wasting padding or distractingly unskilled writing?
Am I entertained, amused, or emotionally motivated in a positive way that makes me want to read more by the same writer?
And for the specific user-provided example above, make sure the author knows the difference between “pared down” and “parsed down” and doesn’t misstate “rev cycle” as “rest cycle.”
From FlyOnTheWall: “Re: Mary Piepenbrink, RN. Joined a startup called Pieces Technologies as SVP of sales. What do you know about them?” I’ve heard of the Dallas predictive analytics company, but only barely. They’re a Parkland Health spinoff as I recall. Founder and CEO Ruben Amarashingham, MD, MBA has good credentials in informatics. The company raised $21.6 million in a single Series A round just over a year ago and apparently has earned a couple of customers.
HIStalk Announcements and Requests
The web hosting company is migrating the site to a bigger server, so let me know if you see anything weird, other than the fact that I’m posting this later than usual to accommodate the switch.
You’ll see some inarguably huge news related to a Meaningful Use-related EHR vendor settlement coming out, possibly as early as later today. The financial terms are mind-boggling. More to come once the Justice Department’s announcement is released.
Listening: The Stanfields, Nova Scotia-based hard-working rockers who wrap thoughtful, lyrically rich biographical stories with searing guitar (and mandolin) riffs. like AC/DC covering an Irish pub’s house band. It’s sonically spectacular poetry. You’re a poser rather a musician if you can’t play and sing acoustically in a bare room, to which I submit the amazing “Vermilion River.”
Webinars
June 22 (Thursday) 1:00 ET. “Social Determinants of Health.” Sponsored by Philips Wellcentive. Presenter: David Nash, MD, MBA, dean, Jefferson College of Population Health. One of the nation’s foremost experts on social determinants of health will explain the importance of these factors and how to make the best use of them.
June 29 (Thursday) 2:00 ET. “Be the First to See New Data on Why Patients Switch Healthcare Providers.” Sponsored by Solutionreach. As patients pay more for their care and have access to more data about cost and quality, their expectations for healthcare are changing. And as their expectations change, they are more likely to switch providers to get them met. In this free webinar, we’ll look at this new data on why patients switch and what makes them stay. Be one of the first to see the latest data on why patients leave and what you can do about it.
July 11 (Tuesday) 1:00 ET. “Your Data Migration Questions Answered: Ask the Expert Q&A Panel.” Sponsored by Galen Healthcare Solutions. Presenters: Julia Snapp, manager of professional services, Galen Healthcare Solutions; Tyler Suacci, principal technical consultant, Galen Healthcare Solutions. This webcast will give attendees who are considering or in the process of replacing and/or transitioning EHRs the ability to ask questions of our experts. Our moderators have extensive experience in data migration efforts, having supported over 250+ projects, and migration of 40MM+ patient records and 7K+ providers. They will be available to answer questions surrounding changes in workflows, items to consider when migrating data, knowing what to migrate vs. archive, etc.
Previous webinars are on our YouTube channel. Contact Lorre for information on webinar services.
Acquisitions, Funding, Business, and Stock
Health management software vendor Mediware Information Systems acquires Kinnser Software, which offers home health and hospice systems.
Two former Theranos board members – former US Navy Admiral Gary Roughead and former US Secretary of State George Shultz – say they didn’t ask founder Elizabeth Holmes about media reports stating that the company wasn’t running many tests on its proprietary Nanotainer finger stick technology but instead was using commercially available analyzers. Legal experts question whether the company’s board failed to meet their responsibilities in providing checks and balances to Holmes, who controls 98.3 percent of voting shares. To paraphrase “Animal House” in work-friendly terms, “You messed up … you trusted us.”
Consumer health information site Sharecare, founded in 2010 by Dr. Oz and WebMD founder Jeff Arnold, receives an unspecified investment from Summit Partners, increasing its total to more than $300 million.
Announcements and Implementations
Google launches the free Data Gif Maker, a data illustration tool aimed primarily at journalists who need to tell data-driven stories but potentially useful to a wider social media audience.
Medisolv chooses CloudWave’s OpSus Healthcare Cloud for making its quality management system available to customers as a SaaS offering.
Nordic announces that it has grown to 700 consultants serving 200 clients.
Reaction Data publishes a new report on patient referrals and self-scheduling.
Government and Politics
The CEO of Blue Cross Blue Shield North Carolina says that the ACA marketplace is stabilizing in price, utilization, and risk to the point that an 8.8 percent premium hike would have sufficed for 2018, but instead the company has filed for a 22.9 percent increase because the White House keeps saying that it may not continue paying the premium subsidies that have been challenged legally. “The information we’ve seen coming from the administration actually creates more uncertainty,” the CEO says.
Privacy and Security
Ascension-owned Seton Healthcare (TX) says it has identified “suspicious activity within our network,” but provided no details, although it sounds like a ransomware attack. Meanwhile, patients report to the local TV station that the hospital has gone back to paper after warning employees to shut down the computers.
Other
A study finds that hospital EDs charge an average of 3.4 times the Medicare-paid rate for services they provide, providing as an example EKG interpretation, for which Medicare pays a median of $16 but for which hospital EDs charge other patients anywhere from $18 to $317, averaging $95. The highest-charging hospitals are for-profit, mostly in the South and Midwest, and serve more uninsured and minority patients.
USA-based Syria medical aid group UOSSM launches Syria Solar, a project to install solar power systems in the country’s hospitals, which run generators that use erratically available diesel fuel. Much of Syria’s electrical grid has been destroyed by bombing, leaving already struggling hospitals to deal with power outages for incubators, dialysis machines, and other vital equipment.
Rapidly rising drug prices are hitting seniors hard with higher co-pays even as Medicare’s share of the Part D cost has become its fastest-growing expense. Novartis AG has raised the price of cancer drug Gleevec 77 percent in the past five years, increasing Medicare’s annual cost from $500 million to $1.23 billion and leaving the average Medicare patient paying $4,400 per year out of pocket.
I’ve read that Europe has become even more overrun with summer tourists in the past few years because huge-population countries like China and India are moving up the economic food chain and their now-wealthier citizens are joining the lines in Rome, Paris, and London. A New York Times article says that’s also true in healthcare, as frustrated, affluent citizens of China are bypassing the country’s overloaded hospital system and paying cash for care in the US and other countries despite the inevitable problems with transoceanic care coordination.
A Wall Street Journal article questions whether towns should continue operating tax-supported nursing homes, seven percent of which are government-owned. Their financial losses are increasing due to a glut of Baby Boomer residents, a high proportion of Medicaid residents as those with more assets seek out tonier facilities, and the White House’s proposal to cut Medicaid by nearly a trillion dollars. Cities are selling their nursing homes to private operators with mixed experience. The article profiles the city-owned, 45-bed nursing home in Cape Cod’s Nantucket, MA, which is losing $3 million per year, needs major repairs as the city grapples with other huge infrastructure upgrades, and attracts only the financially struggling year-round residents who would have to move out if the city’s only nursing home shuts down or raises rates.
Sponsor Updates
AdvancedMD publishes a MIPS Improvement Activities fact sheet.
Aprima will exhibit at the Associated Professional Sleep Societies Annual Meeting June 5-7 in Boston.
Audacious Inquiry publishes a series of white papers on what HIOs need to know about the 21st Century Cures Act.
Bernoulli publishes a new case study, “Achieving medical device connectivity across a multiple-hospital enterprise.”
Datica will present at the Wisconsin Entrepreneurs’ Conference June 6-7 in Madison.
Carevive Systems will exhibit at the ASCO Annual Meeting June 2-6 in Chicago.
Casenet will exhibit at AHIP Institute & Expo June 7-9 in Austin, TX.
Docent Health is featured in Redox’s “Digital Health Done Right” series.
The Jacksonville Business Journal includes CSI Healthcare IT in its list of “Best Places to Work 2017.”
Dimensional Insight will host its annual User Conference June 5-8 in Boston.
In Canada, a report by Alberta’s auditor general says the government’s $1.2 billion proposed project to replace the clinical and administrative systems of Alberta Health Services with a single system is not likely to generate the expected $900 million in cost savings because it doesn’t include primary care practices.
The project, announced a year ago, would replace 1,300 individual AHS systems.
The report notes that Albertans pay the highest healthcare costs of all provinces in Canada, yet the quality and integration recommendations of previous reports have been mostly ignored. It observes that despite claims of how good healthcare is in Canada, it’s almost as bad as in the US, which finishes dead last among 11 developed countries despite spending far more than any of them.
The Auditor General also notes that fee-for-service payments have hampered accountability and integration. It also says that health leader turnover is high due to political cycles, with the average AHS hospital CEO lasting just 1.2 years.
Province physicians use at least 12 incompatible EHRs. Canada-wide, 94 percent of hospitals use IT only for administrative tasks.
The report observes that if banks used IT like Alberta Health Services:
Each branch bank would have its own systems that can’t communicate with other branches.
Systems at some branches would be so prone to failure that paper files would be kept ready.
Tellers, mortgage officers, and investment specialists wouldn’t be able to access each other’s information.
The only access to banking information would be via faxing.
Customers would be required each time they visit a branch to fill out the same form asking for name, address, employment information, and financial history.
Traveling customers could not withdraw money without opening an account first because the branch would not know who they are.
Applying for a mortgage would require visiting each prospective lender individually and completing their proprietary application package.
Online banking would not exist.
Obtaining an account balance would require making a written request and waiting two weeks for the mailed information to arrive.
Bank managers would not have enough information to understand the performance of individual branches.
The banks would spend $600 million per year to maintain IT systems but without a plan to standardize them and keep them up to date.
Reader Comments
From More Math: “Re: CommonWell’s 60,000 documents downloaded. Looking at the latest from Epic’s website, it appears that Care Everywhere hits CommonWell’s lifetime exchange number every 15 minutes. Sounds like Epic is willing and able. Bigger question is whether the CommonWell is drying up.” CommonWell’s March 2017 fact sheet says that 5,100 provider sites have gone live and have generated 85 million queries, although I don’t know how “queries” translates into “documents.” The quoted figure of 60,000 documents retrieved doesn’t indicate the time frame involved, but if that’s all of them since CommonWell’s beginning in 2013, that’s a pretty anemic number. Cerner said in a HIMSS16 presentation that it had 4,000 providers live on CommonWell, which suggests that almost all live CommonWell members are Cerner users; that those providers enrolled only an average of 50 patients each; and that only eight documents per provider were actually retrieved. EHR vendors pay a per-transaction cost to CommonWell and providers don’t really like sharing their patient information with competitors, so there’s not a lot of economic incentive for anyone other than the patient to use CommonWell’s services.
From Laura Palmer: “Re: Cure Forward. Has shut down, according to its site.” The Boston startup offered a platform that matched patients with clinical trials, although previous announcements suggest that its system may never have graduated from beta testing status. The company raised $19 million in a June 2015 investment and nothing since. Sole investor Apple Tree Partners has expunged Cure Forward from its website, omitting the company from its “legacy investments” section and removing previous Cure Forward press releases (thereby practicing the investing world’s legendary 20-20 hindsight). Cure Forward founder Martin Naley, who launched the company as a entrepreneur in residence at Apple Tree Partners, says on his LinkedIn profile that the company “ceased operations at the end of May 2017 due to financing difficulty.”
HIStalk Announcements and Requests
Readers funded the DonorsChoose grant request of Mrs. M in Ohio, who requested math fluency games and fitness-related “brain breaks.”
Two-thirds of the 247 poll respondents who say they have certification or fellowship credentials don’t list them on their business cards or in their email signatures. KG says credentials should be listed only on CVs other than for practicing clinicians, while Sue says her earned credentials are important to her work and her clients use them as well. John opines that healthcare people deploy “a fruit salad of acronyms” such that the more of them someone lists, the less he believes what they say.
New poll to your right or here: to what extent has CommonWell benefited patients since its 2013 founding? I appreciate your vote and, even more so, your comments explaining it.
Gregg Allman died Saturday at 69, leaving zero of the two brothers who founded the Allman Brothers Band in 1969 still alive (also making Cher the ex-wife of two deceased celebrities). I’m not a fan at all of the retired band’s music since I really dislike Southern boogie and country music even when it’s bluesy (other than Lynyrd Skynyrd, anyway), but it’s apparent that hard living took its toll on the founding members — Duane Allman died at 24 in 1971 in a motorcycle accident, bass player Berry Oakley died a year later in the same manner and location, and drummer Butch Trucks killed himself earlier this year. That leaves guitarist Dickey Betts (73) and drummer Jaimoe Johanson (72).
I’ve had problems for years where I leave the laptop running and Firefox is open to pages that refresh (like Twitter or news sites) – Firefox gets sluggish and Windows Task Manager shows it eating up a huge amount of memory and CPU, requiring me to hard-cancel it. The solution – I finally switched to Chrome for everything browser related, which makes even more sense now that I’m using a Chromebook and an Android phone. My only non-Google technology is an iPad Mini and the Windows laptop, both of which will move to a Google platform when it’s time to replace them.
In Flanders Fields By John McCrae, MD (1872-1918)
In Flanders fields the poppies blow Between the crosses row on row That mark our place; and in the sky The larks, still bravely singing, fly Scarce heard amid the guns below.
We are the Dead. Short days ago We lived, felt dawn, saw sunset glow, Loved and were loved, and now we lie In Flanders fields.
Take up our quarrel with the foe: To you from failing hands we throw The torch; be yours to hold it high. If ye break faith with us who die We shall not sleep, though poppies grow In Flanders fields.
This Week in Health IT History
One year ago:
Forbes revises its estimate of the net worth of Theranos founder Elizabeth Holmes from $4.5 billion to zero.
An ONC study finds that 84 percent of US hospitals are using at least a Basic EHR, a nine-fold increase since HITECH’s adoption in 2009.
DrFirst acquires Meditech-focused consulting firm The IN Group.
CHIME awards $30,000 each to the two finalists in the concept round of its national patient ID challenge, with those contestants moving to the final $1 million round.
Five years ago:
Allscripts caves in to a proxy fight and adds three new board members advocated by key shareholder HealthCor Partners, which had publicly called for Allscripts to fire CEO Glen Tullman.
Three-fourths of respondents to my poll disagree with Neal Patterson’s assertion that Cerner and Epic will end up being the only hospital EHR survivors.
Fired HCA doctors say the hospital chain hired huge numbers of physicians to prepare for an ACO environment, then terminated those whose practices weren’t profitable.
Ten years ago:
A research article finds that few hospitals are using bedside barcode-checking of medications and that nurses bypass those systems frequently.
An article describing problems with Kaiser Permanente’s shuttered kidney transplant program blames information management problems and its paper-based systems.
A rumor suggests that Misys is trying to sell its hospital systems.
Former National Coordinator David Brailer launches the $700 million private equity fund Health Evolution Partners.
MED3OOO takes a majority ownership position in InteGreat.
This week’s survey: what is the role of the person you most value as a mentor and/or professional peer, how did you connect with them, and how do you maintain the relationship?
Last Week’s Most Interesting News
The Wall Street Journal notes that uncertainty surrounding the Affordable Care Act has forced some health IT startups to change their strategies.
Five hospitals in Australia experience an IT incident cause by applying security patches to protect against WannaCry ransomware.
Apple acquires sleep monitoring sensor and app vendor Beddit.
The Congressional Budget Office estimates that the Affordable Health Care Act would increase the number of uninsured Americans by 23 million by 2026 in reducing the deficit by $119 billion.
The Bipartisan Policy Center calls for private-public efforts to improve health IT safety, but does not mention ONC’s proposed EHR safety center.
The director of Denmark’s equivalent of the FDA warns that big US tech companies like Google and Apple are rolling out health apps without demonstrating their efficacy and safety and that those companies are gaining permanent access to patient data.
The local paper says that Erie County Medical Center’s ransomware infection is still affecting the hospital six weeks after the hospital decided not to pay the demanded $44,000 ransom, also running a screenshot provided by a hospital employee that suggests that the culprit was Samas, the same malware that took down MedStar Health in 2016.
Webinars
June 22 (Thursday) 1:00 ET. “Social Determinants of Health.” Sponsored by Philips Wellcentive. Presenter: David Nash, MD, MBA, dean, Jefferson College of Population Health. One of the nation’s foremost experts on social determinants of health will explain the importance of these factors and how to make the best use of them.
June 29 (Thursday) 2:00 ET. “Be the First to See New Data on Why Patients Switch Healthcare Providers.” Sponsored by Solutionreach. As patients pay more for their care and have access to more data about cost and quality, their expectations for healthcare are changing. And as their expectations change, they are more likely to switch providers to get them met. In this free webinar, we’ll look at this new data on why patients switch and what makes them stay. Be one of the first to see the latest data on why patients leave and what you can do about it.
July 11 (Tuesday) 1:00 ET. “Your Data Migration Questions Answered: Ask the Expert Q&A Panel.” Sponsored by Galen Healthcare Solutions. Presenters: Julia Snapp, manager of professional services, Galen Healthcare Solutions; Tyler Suacci, principal technical consultant, Galen Healthcare Solutions. This webcast will give attendees who are considering or in the process of replacing and/or transitioning EHRs the ability to ask questions of our experts. Our moderators have extensive experience in data migration efforts, having supported over 250+ projects, and migration of 40MM+ patient records and 7K+ providers. They will be available to answer questions surrounding changes in workflows, items to consider when migrating data, knowing what to migrate vs. archive, etc.
Previous webinars are on our YouTube channel. Contact Lorre for information on webinar services.
Acquisitions, Funding, Business, and Stock
Debt-ridden Florida-based clinic operator 21st Century Oncology – which was breached by hackers in 2016 in exposing the records of 2.2 million patients and resulting in at least 13 federal class action lawsuits – files Chapter 11 bankruptcy. As companies tend to do, 21st Century calls the bankruptcy a “positive development,” brags that it is “fundamentally strong and profitable,” and claims that “very little, if anything, should change during the Chapter 11 process,” calling into question either the credibility of the company or of the US bankruptcy process that is often used as a shrewd corporate strategy to legally screw employees and creditors for the benefit of executives.
Decisions
Fitzgibbon Hospital (MO) will replace Meditech and GE Healthcare with Cerner in November 2017.
Pinnacle Hospital (IN) will go live with Prognosis Innovation Healthcare in June 2017.
Illinois Valley Community Hospital (IL) will implement Athenahealth’s EHR in November 2017, replacing McKesson.
Pioneers Medical Center (CO) will go live with Athenahealth in 2017.
Riverside Tappahannock Hospital (VA) will replace Siemens with Epic in June 2017.
These provider-reported updates are supplied by Definitive Healthcare, which offers a free trial of its powerful intelligence on hospitals, physicians, and healthcare providers.
Announcements and Implementations
Vanderbilt LifeFlight develops an Uber-like app to allow first responders to request a helicopter, sending the service an the GPS coordinates and and requestor information while giving the emergency responder a real-time flight map and estimated arrival time.
Other
A co-founder of startup Iodine — which published patient-submitted experience with medications — says his company, as well as other digital health startups, were naive in thinking that their technology could create a healthcare revolution. Iodine quietly sold itself off to drug discount coupon publisher GoodRx a few months ago. Thomas Goetz says not only did disruption not happen, it probably never will, because:
Entrenched players are huge and have their hands in multiple aspects of healthcare.
Nobody cares about better-faster-cheaper in healthcare.
There’s no ability to shop prices.
The government is the biggest customer.
Incentives are misaligned.
The Columbus, OH paper profiles prescription prior authorization system vendor CoverMyMeds, the first local startup to sell itself for at least $1 billion (to McKesson in January of this year for $1.1 billion, this case). CEO Matt Scantland says the company’s formula for success was, “Start with a big problem and solve it not by disrupting anything, but by finding a way that everyone wins,” adding that it wasn’t the first company to tackle the problem, but rather the first to develop a scalable solution. The article notes that CoverMyMeds has over 500 Columbus-based employees who get a free gourmet lunch each day and have a virtual reality room to play video games with peers in its Cleveland office. I interviewed Matt in September 2014 when the company had just 73 employees and $19 million in revenue, but he was predicting bigger things:
Prior authorization seems like a very niche thing. It kind of is, but at the same time, it’s also right at the intersection where a doctor is making a decision about the tradeoffs between the cost of a treatment and its efficacy. We think that that’s a fundamental problem in healthcare. We have built both the network and the connectivity and then also the relationships with pharma, payers, pharmacies, and providers. We think we can help doctors make more intelligent consumption decisions. We think is a very large opportunity, starting with drug, but helping to get to more personalized medicine in terms of prescribing, and then also other procedures as well. Because of the growth of the size now, we have a lot of interest from the financial and strategic partners. We’re always willing to listen. We think this is a very big standalone company on its own.
He went down, under. In Australia, a member of Parliament laughs so hard while watching the US TV show “Veep” that he chokes on his sushi, passes out, and stumbles through his house before falling face-down unconscious into his granite kitchen island, leaving him with a black eye, three stiches, and a get-well tweet from star Julia Louis-Dreyfus.
Sponsor Updates
Encore, A Quintiles Company publishes a white paper titled “Care Management Framework – The Critical Path to Implementing a Care Management Strategy.”
QuadraMed, a Harris Healthcare company, will exhibit at the NYHIMA Annual Conference June 4-7 in Rochester.
Salesforce announces strategic agreement with Dell Technologies.
Solutionreach expands leadership team with new promotions.
Summit Healthcare and Access will exhibit at the 2017 International MUSE Conference May 30-June 2 in Dallas.
May 27, 2017NewsComments Off on Reader Survey Results: Job Promotion Factors
I asked what factors affected a job promotion.
Being humble, but speaking up in meetings (especially with solution ideas for important problems).
Many factors worked together to promote me through three levels in five years. An ability and willingness to drive change and tackle challenges in areas traditionally labeled as “impossible” because they required revamping entrenched negative habits. An unflinching determination to get tasks done on time (with no short cuts) and work out compromises even with the most difficult stakeholders. The ability to get to the root cause of an issue and focus on how to avoid future snafus with education and documentation without dwelling on placing blame. Consistently keeping EVERYONE very well aware of a projects progress and problems – so everyone felt in the know. Taking copious and diligent notes so as to instill trust and confidence when making statements at meetings, allowing decision makers to move forward more quickly. It also didn’t hurt getting another master’s degree specializing in a key niche area! Never let your skills become stale or your attitude become obstinate.
Proving myself works in getting more responsibilities. Moving to a new company was required to get a promotion.
Paying attention. I don’t believe in random luck, I believe that if you keep your mind open, you will be able to see the opportunities that are all around you. Luck is the ability to see the doors that are already open, waiting for you to step through. Also, be kind and generous.
I do not seek a promotion as something to have, a title to add to my business card or resume. I do not seek a promotion as a reward for time served or deeds already done. I seek a promotion for the opportunity to connect with new people to share ideas, the ability to move forward with new kinds of projects, the ability to tap into new resources. If you can articulate your desire for promotion in the context of moving forward instead of looking backward (a reward) or appearance (new business cards), then your organization will see you as a part of their future as well.
Always doing what I think is the right thing,and the best things for my customers. Always be honest and when I see a problem or an opportunity for improvement, regardless if I am responsible for it or not, I try to identify a solution.
Not looking for the promotion and focusing on making my boss(es) look good. Supporting their ideas and approaches.
I’ve had three offers to get a significant bump in salary and/or role. Every time was when I threatened to quit.
Receiving offers from other companies willing to pay me more.
Job changes, willingness to take on new projects, show value and communicate it.
Building relationships and consistently delivering results.
Who you know and certifications. Also geographical location seems to be a factor — if the person who is doing the hiring is from the same area of the country as you, then that helps with a connection.
Being better at the job than all the other people around me.
I’m a white male. I am also smart, talented, and hard working. But judging from my colleagues, being a white male is often all that is needed to climb the ladder. Competency does not seem to be a requirement.
A good boss. There are ideas, and there is doing. Do. Prompt responses to your boss and your boss’s boss.
#1: Asking for them. Having competing offers (that helped with salary level). Having (at the time) a relatively unique background with IT and medical experience. Having the right networks of people who give your request credibility
Company laid off one-third of people. We all applied elsewhere, they begged us to stay. To stay, I requested improved salary, vacation, and title. They obliged.
Leaving.
Most of my promotions have occurred when I’m working for someone who gets things done and cares about my career. Lesson: Think about who you are aligned with professionally.
Self-sufficiency and a willingness to figure things out on my own.
The ability to lead others, even if not in an appointed leadership role. Last promotion to Lead Analyst role earned by demonstrating ability to assist new and current co-worker analysts to achieve positive results. Sometimes though one is born with an innate nature to lead and enjoy doing so (without be overbearing – i.e., “bossy”). One can always possess a technical ability to perform job duties, but needs guidance and mentoring to achieve success.
My ability to smile while professionally dealing with the jackasses that infest our fine HIT industry.
Being a woman. Just kidding!
My top 3: specific measureable business results from work. The ability to communicate effectively with both non-IT and IT people. Reasoned risk-taking.
Integrity, dedication to performing at the best of my ability, and respect for everyone’s role and contribution to delivering quality services.
Being in the right place at the right time. Having a track record of delivering results. Being helpful and useful. Thinking critically and anticipating my next action. Dressing nice, being well groomed and presentable, speaking clearly and confidently, having a sense of humor, and being able to relate to everyone, not just my peers.
The uncertain future of the Affordable Care Act is forcing some health IT startups – especially those that sell mostly to hospitals – to change their strategies, according to a Wall Street Journal report.
The political turmoil has also raised the funding bar as investors seek out companies with solid revenue and market validation, thereby putting their money into fewer but larger deals.
These companies are reported to have made changes due to ACA uncertainty:
Smart pill bottle maker Pillsy is refocusing its sales efforts on consumers rather than providers.
Diabetes management technology vendor Omada Health is increasing its sales emphasis on clinical evidence and return on investment.
Pregnancy tracker app vendor Babyscripts is concentrating on large health systems instead of physician practices.
Take Command Health, which helps people who can’t get employer-provided health insurance find coverage, is revamping its platform to target small businesses that reimburse employee healthcare costs.
Amino, whose tools target specialty care, raised $25 million after changing its platform to analyzing the cost of preventive services that may no longer be free with ACA changes.
Reader Comments
From Ex Epic: “Re: CommonWell. In the Madison consultant community, it’s pretty much understood that CommonWell is/was a Cerner marketing campaign to win the DoD. They tweeted these numbers at their collaboration forum last week, with quick math showing they have roughly one document retrieved per customer facility.”
HIStalk Announcements and Requests
This week on HIStalk Practice: Solutionreach’s Jim Higgins highlights the importance of patient relationship management in attracting and keeping millennial patients. Qliance Medical Management abruptly shuts down clinics amidst financial and legal difficulties. Lemonaid Health raises $11 million. Harbin Clinic adds PrecisionBI analytics to its Athenahealth tools. School nurses up in arms over incentivized telemedicine consent. Femwell Group Health will offer HealthGrid patient engagement tech. ClearHealth Quality Institute looks for telemedicine committee candidates.
Webinars
June 22 (Thursday) 1:00 ET. “Social Determinants of Health.” Sponsored by Philips Wellcentive. Presenter: David Nash, MD, MBA, dean, Jefferson College of Population Health. One of the nation’s foremost experts on social determinants of health will explain the importance of these factors and how to make the best use of them.
June 29 (Thursday) 2:00 ET. “Be the First to See New Data on Why Patients Switch Healthcare Providers.” Sponsored by Solutionreach. As patients pay more for their care and have access to more data about cost and quality, their expectations for healthcare are changing. And as their expectations change, they are more likely to switch providers to get them met. In this free webinar, we’ll look at this new data on why patients switch and what makes them stay. Be one of the first to see the latest data on why patients leave and what you can do about it.
July 11 (Tuesday) 1:00 ET. “Your Data Migration Questions Answered: Ask the Expert Q&A Panel.” Sponsored by Galen Healthcare Solutions. Presenters: Julia Snapp, manager of professional services, Galen Healthcare Solutions; Tyler Suacci, principal technical consultant, Galen Healthcare Solutions. This webcast will give attendees who are considering or in the process of replacing and/or transitioning EHRs the ability to ask questions of our experts. Our moderators have extensive experience in data migration efforts, having supported over 250+ projects, and migration of 40MM+ patient records and 7K+ providers. They will be available to answer questions surrounding changes in workflows, items to consider when migrating data, knowing what to migrate vs. archive, etc.
Previous webinars are on our YouTube channel. Contact Lorre for information on webinar services.
Acquisitions, Funding, Business, and Stock
Clinical trials software vendor Medrio receives a $30 million equity investment from Questa Capital Management.
Apple acquires Finland-based Beddit, which offers a sleep tracking app that uses mattress-attached flexible sensors.
People
Jessica Campbell (Leidos Health) joins Nordic as VP of client partnerships.
Announcements and Implementations
Elsevier will add its ClinicalKey clinical search engine to the World Health Organization’s Research4Life journal access program for developing countries.
The DiamondView HIE of South Country Health Alliance (MN) goes live with Medicity Notify, which provides electronic notification services for population health management that will be rolled out across its 11 counties.
Government and Politics
ProPublica reports that some Republican lawmakers who are being called out on social media for their support of the American Health Care Act (and their sometimes incorrect statements about it as copied and pasted from White House talking points) are blocking their vocal constituents on social media after deleting their comments. An example is Congressman Peter King (R-NY), who not only appears to be censoring critical comments, but is also declining to conduct in-person town hall meetings because attendees scream at him.
Privacy and Security
In Australia, Queensland Health experiences a major EHR failure after applying WannaCry security patches from Microsoft, Cerner, and Citrix that slowed down systems and affected the ability of users to log on.
A survey finds that only 9 percent of medical device manufacturers test the security of their products at least once a year, with nearly half saying they don’t perform security testing at all. One-third of both manufacturers and health systems say no single person is in charge of device security and half say they don’t follow the FDA’s guidance to reduce security-related risk.
A security researcher finds that medical claims processed by insurer Molina Healthcare were freely accessible over the Internet simply by changing the number at the end of any claim’s URL to bring up a different claim, with no authentication required. The company fixed the problem after being notified and has shut down its portal pending a security review.
Other
NantHealth CEO Patrick Soon-Shiong announces plans to open a cancer center, saying that the city has a great basketball team and newspaper (he owns a chunk of both), but not a great cancer center.
Slides from Cerner’s investor conference presentation show that Cerner and Epic (which Cerner references by name, which doesn’t happen often) each hold 24 percent of the acute EHR market. Cerner won decisions involving 109 hospitals in 2016 vs. Epic’s 91, although it was 69 vs. 66 when excluding existing customer add-ons. It also notes that 2,400 hospitals are using legacy systems that offer a replacement opportunity, with more than one-fourth of them running Meditech Magic or C/S.
A group from Kaiser Permanente writes a Harvard Business Review article about KP’s efforts to get surgery patients out of the hospital quicker by using standardized processes and team coordination. The authors honor Jess Jacobs, who at the time of her death in 2014 at 29 had measured that in her 20 ED visits, 54 inpatient days, and 56 outpatient visits, only 0.08 percent of her time was spent actually treating her medical problems.
The State of New Jersey temporarily suspends the medical license of a psychiatrist who had prescribed thousands of doses of oxycodone for a single patient, with the attorney general announcing, “Our message to these doctors is clear: if you are not checking the Prescription Monitoring Program database as required by the new law, we will take swift and punitive action against you.”
The Wall Street Journal profiles CVS Health EVP/CIO Stephen J. Gold, who says that 30 percent of the company’s pharmacy customers use its text messaging system for prescription refills. He mentions CVS’s Fast Mobile Prescription Pickup, which allows customers to pick up their refills at the counter or drive-through by scanning the barcode sent to their phones. The company is also using a proprietary health engagement engine to look for intervention opportunities, such as sending a message to patients who aren’t taking medications as prescribed or reminding diabetics to test their blood glucose. Another CVS digital tool allows patients to synchronize the refills of all of their prescriptions to save a trip and to improve adherence.
The State of Minnesota, admitting that it can’t keep up with complaints about nursing homes that mistreat their residents, warns nursing homes that they cannot harass families who install “granny cams” in the rooms of residents to document the care their loved one receives. The ruling came after a woman who had placed a $199 video camera in her mother’s room complained that nursing home employees frequently covered it with a towel, unplugged it, pressured her mother to remove it by refusing to speak to her when entering her room, and eventually seized it.
The US finishes in its customary back-of-the-pack spot in a new global health measure that looks at: (a) how well countries prevent deaths by applying known medical interventions; and (b) how health measures improve with increasing national wealth. The author says it’s “an embarrassment” that the US spends $9,000 per citizen annually on healthcare while failing to improve its lagging world health position.
Sponsor Updates
The Chartis Group publishes a white paper titled “Performance Transformation: An Undeniable Requirement in Uncertain Times.”
GE Healthcare previews its upcoming film, “Heroines of Health.”
Meditech announces that it sold systems to five customers representing 16 hospitals in Q1.
EClinicalWorks will exhibit at the 2017 MPHCA Annual Conference May 30-June 2 in Biloxi, MS.
The Bipartisan Policy Center calls for creating a public-private effort to set health IT safety priorities and to disseminate best practices.
The report recommends:
General patient safety efforts should incorporate the safety of health IT throughout its life cycle.
Health IT safety should be addressed via a non-punitive learning system similar to medical error reporting.
Voluntary and mandatory reporting systems should collect de-identified data about health IT safety issues that can drive creation of evidence-based practices and tools.
The report does not specifically address ONC’s proposed EHR safety center.
Reader Comments
From Vaporware?: “Re: Cerner. How long do they get a free pass on selling interoperability without delivering? Beth Israel Deaconess Care Organization lists just six EHRS of the 40 its providers use – Cerner not among the six – that are willing and able to contribute information to its population health analytics system. Do the live MHS Genesis pilot sites have connectivity to outside EHRs?” I’ll invite readers with the firsthand experience with either project that I don’t have to comment anonymously.
From Chaste Kiss: “Re: this HIMSS-owned publication’s story. I’m embarrassed that I actually clicked the tweet to read more.” No wonder – you were cheated when a publication runs a story titled “Is a takeover of Athenahealth inevitable?” that doesn’t actually answer the question it poses (nor could it). It simply rewords a lazy Bloomberg opinion column in which those original authors speculated –without using any sources or providing evidence of analytical thought — that maybe Cerner, IBM, UnitedHealthGroup, Aetna, or Epic might be interested in buying Athenahealth (the fact that Epic was named means the authors are clueless). The embarrassingly lazy source article wasn’t improved one iota by having the HIT publication improperly legitimize it by rephrasing its undisciplined conclusions. In both cases, the writers seemed desperate to fill their allotted space with whatever fizzy “news” they could make up with a minimum of expended effort.
From Greg: “Re: sepsis monitoring. The new Meditech 6.1 Surveillance product has a rules-based approach that looks at real-time EMR clinical data in the EMR. There the clinician can be notified and take appropriate action in an efficient and sometimes life-saving manner. These actions can include orders, medications, labs, documentation, problems, interventions, etc. I have personally not seen another EMR that is as far advanced with regards to surveillance.”
From SgtPerkins: “Re: John Brownstein’s tweet about Epic’s App Orchard developer terms. It is no longer available. $50 says he got a C&D from Epic to remove it. Even their awful legalese is intellectual property to them.” Unverified. My screenshot of his tweet from the Boston Children’s chief innovation officer is here. My experience is that such takedown requests often come from an individual’s employer rather than the subject of their comments, especially when the employer is a partner of the company mentioned (as I well know, having been threatened in my early, less-anonymous HIStalk days with being fired by my hospital employer for writing about one of our vendors even though it wasn’t inside information). Also, Epic’s App Orchard legal wording wasn’t really a secret anyway since it’s publicly available and, as other readers have noted, is similar to that of the Apple Store.
HIStalk Announcements and Requests
Readers funded the DonorsChoose grant request of Mrs. D in Arkansas, who asked for writing journals and math activity kits and games for her elementary school class. She reports, “These materials have allowed students to learn using a hands on approach. We love all of our games and our writing journals! Students are so proud to have their own journal to write in each day. You have made all the difference! Thanks again.”
Webinars
None scheduled soon. Previous webinars are on our YouTube channel. Contact Lorre for information on webinar services.
Acquisitions, Funding, Business, and Stock
Post-acute care software vendor Optima Healthcare Solutions acquires Hospicesoft, which offers hospice software.
Sales
Five Ontario hospitals add PatientKeeper CPOE and medication reconciliation to their existing system and will expand their use of the company’s physician documentation solution, providing an overlay to Meditech Magic and other systems.
St. Joseph Health (CA) will expand its use of Clearsense analytics in implementing Inception for archiving, access, and visualization of its legacy Meditech data.
Harbin Clinic (GA) chooses analytics from PrecisionBI, a division of Meridian Medical Management.
People
A Philadelphia innovation organization recognizes Children’s Hospital of Philadelphia AVP/Chief Health Informatics Officer Bimal Desai, MD, MBI as its healthcare innovator of the year. He co-founded CHOP spinoff Haystack Informatics, which offers security technology that detects EHR snooping by learning normal staff behavior and calling out exceptions.
Rush Health (IL) launches Rush Health Connect, which aggregates information from its Epic and Allscripts EHRS using InterSystems HealthShare to give clinicians patient information and real-time alerts and notifications.
Change Healthcare joins the Hyperledger open source blockchain project.
The Fresno paper covers the use by Community Medical Centers of RightPatient iris recognition at patient registration, which the article explains isn’t an infrared scan, but rather just a photo of the patient’s eye. It also notes that palm vein ID systems are an alternative. RightPatient can also analyze a patient’s general headshot to identify them going forward.
DrFirst will integrate prescription pricing information from GoodRx into its e-prescribing platform.
Government and Politics
A VA OIG suicide prevention report finds that around 20 percent of inspected VA facilities don’t perform the mandated five outreach events per month, haven’t developed suicide prevention safety plans that are documented in the EHR, and don’t flag high-risk patients in the EHR. More alarmingly, OIG found that while 84 percent of non-clinical hospital hires completed their mandatory suicide prevention training within 90 days, nearly half of newly hired clinicians did not do so.
The director of Denmark’s version of the FDA expresses concern that US tech companies like Google and Apple are rolling out medically-related fitness tools and devices that “have no requirements to demonstrate efficacy and safety, but we are forced into the direction of taking them seriously.” The finance minister warns that while patients are notified by email any time their Denmark-based interoperable electronic medical records are viewed, private services and apps offer no such protection, explaining, “We need to make our citizens aware that there is no free lunch with these big companies. People should make some more demands when they give their data away. These companies want to know what you want before you know it yourselves. We need to look into regulation. These private companies will have this patient data for eternity. Can we be sure they’ll always do good things with it?”
A report by HHS’s Office of the Assistant Secretary for Planning and Evaluation blames the Affordable Care Act for the 105 percent jump in premiums from 2013 to 2017 in the 39 states participating in Healthcare.gov, as the average monthly premium increased from $224 to $476. The report, however, didn’t look at the increase in non-exchange sold individual plans and admits in its “Limitations” section that much of the premium increase is probably due to older, sicker people signing up in 2017 vs. 2013. The analysis also fails to note that pre-ACA policies (Healthcare.gov went live in 2013) were often full of coverage loopholes, exclusions, lack of coverage for pre-existing conditions, and lack of insurer experience with an uncertain risk pool.
HIMSS complains about President Trump’s proposed federal budget that calls for major funding cuts for ONC, CDC, CMS, and NIH along with zero money for AHRQ, which would likely be rolled into NIH. The proposal also calls for cutting Medicaid by $800 billion over 10 years.
Other
A Spok survey of 100 hospital CIOs finds that 40 percent of hospitals don’t discipline staff members who violate mobile policies, 30 percent say a significant portion of hospital data is shared insecurely, and more than half of doctors and nurses are unhappy with the communications methods available outside their EHR. Forty-one percent of hospitals don’t offer secure texting and those that do are equally split between providing it via the personal devices of employees vs. hospital-issued technology. Nearly one-third of clinical staff can’t receive clinical alerts or mobile messages from colleagues. CIOs say their hospitals are still using pagers because they are appropriate for some groups, are reliable, and are cheap and easily supported. More than half of the respondents say their biggest challenge in protecting hospital data is a lack of money and people.
A ProPublica investigative piece observes that the still-increasing US maternal death rate is the highest in the developed world and 60 percent of those fatalities are preventable, profiling NICU nurse Lauren Bloomstein, who died of preeclampsia shortly after giving birth in which hospital medical errors apparently contributed. Factors include women giving birth later in life when their medical histories are complex, the nearly half of US pregnancies that are unplanned, the complications of C-sections, and the fragmented health/insurance system that makes it hard to get prenatal care (likely to get worse with any cutbacks to Medicaid, which pays for nearly half of US births). The article notes that perhaps the healthcare system is focused so much on saving the lives of babies – which it has done well – that it isn’t paying enough attention to the health of the mother. A standardized approach to quickly reacting to possible preeclampsia reduced UK maternal deaths to just two in three years, while up to 70 US mothers die of it annually even as US hospitals push back on implementing evidence-based processes.
All you need to know about US health insurance is contained in this one story. An Army veteran whose wife requires pregnancy-related injections not covered by their medical insurance finds that they make $70 too much per month to quality for Medicaid, so they move from North Carolina to Alabama for a job that offers better insurance. He pays COBRA to cover the one-month lapse before their new insurance kicks in. The baby came in early, the NC insurance wouldn’t pay since Alabama is out of network, and the couple gets a bill for a two-week NICU stay for $178,000, of which neither insurance would pay a penny. They can’t get loans and he will lose his defense-related job if they file bankruptcy. They raised a few thousand dollars in a GoFundMe campaign and are hoping to work out a hospital payment plan for the balance that will probably last the rest of their lives.
Instead of the help desk tech term PEBCAK (problem exists between chair and keyboard), this was PEBCASW (steering wheel). In China, a car show model who is demonstrating Nissans’s emergency braking system by standing in front of the moving car is run over (with only minor injuries despite being thrown 10 feet) after the demo driver – who was not familiar with the system – pushes its button twice, turning it on and then off again.
Sponsor Updates
Docent Health assembles bags and lunches for Boston-based charity Bridge Over Troubled Waters.
The American Association of Critical Care Nurses chooses Kathy Douglas, RN, MHA, chief clinical officer of Abililty Network’s ShiftHound, for its Pioneering Spirit award.
CSI Healthcare IT provides at-the-elbow support for MaineHealth’s Epic go-live.
Besler Consulting releases a new podcast, “Lessons learned from the introduction of a physician incentive compensation plan.”
Spok executives will speak at several industry events.
Direct Consulting Associates will exhibit at the SIIM Annual Meeting June 1-3 in Pittsburgh.
The American College of Radiology – a National Decision Support Co. partner – wins the ABIM Foundation Creating Value Challenge for its Radiology-Teaches initiative.
May 21, 2017NewsComments Off on Monday Morning Update 5/22/17
Top News
A Buffalo News report describes the ransomware infection of Erie County Medical Center (NY), from which the hospital has still not fully recovered six weeks later. The hospital declined to pay the $44,000 demanded because it had backups, users could look up patient information from the HealthLink HIE, and administrators worried that the hackers might not restore its files even if the hospital paid up.
The hospital thinks hackers used a brute force password attack to gain control of a hospital Web server a week before the attack, then manually logged on looking for files to encrypt. Clinical systems weren’t restored until a month later.
A hospital-provided screenshot of the ransomware message suggests that the malware is Samas, in which hackers use a variety of tools (including login-stealing malware) to gain credentials and install programs that use Active Directory to propagate the malware to all attached devices.
MedStar Health fell victim to Samas in March 2016 days after both Microsoft and the FBI issued public warnings of its threat. The malware requires online access to just one vulnerable server, often one that’s running unpatched Red Hat JBOSS middleware.
Reader Comments
From Identity Thief: “Re: CHIME’s patient ID challenge. Is anyone questioning its usefulness? The $1 million winner has to provide their solution to the market free of royalties, which means they can’t use any underlying technology that isn’t free. Also, the challenge is based on authentication rather than identity assurance. From NIST, ‘authentication’ implies confirmation of the patient’s presence using authentication factors, while ‘assurance’ means verifying that the person presenting those factors is in fact who they say they are. The solutions of the finalist appear to focus on using tokens (most likely biometric) to authenticate themselves. But before a token can be used, there is a need to identify the patient via inspection of their documents, verifying via a third party , or conducting KBA activities. The FY17 Omnibus legislation requires a strategy that is more than just the pervasive use of an authenticator. It requires a way to roll out a program nationally for all patients and to link a known patient to all of their records from any location in which they have received services. We should question whether a winning authentication solution truly solves the patient identity problem. In my opinion, it does not.” I agree that someone would need to physically verify a person’s identity in issuing their authentication token, but then there’s the question of how a different provider would connect to that information collected elsewhere (perhaps it would be self-contained, like a fingerprint profile stored on a smart card.) As you said, positive identification doesn’t necessarily imply data sharing, but that doesn’t seem to be part of the conversation despite the NIST definition. I would be happy with a solution that would (a) prevent identity fraud; and (b) give hospitals a single ID that would eliminate patient merges and that would link all of a patient’s information even just within that one organization’s systems.
From Arm Twister: “Re: Athenahealth. They say they have 35 MU attestations using their complete inpatient solution, but CMS shows only 17 inpatient attestations. Also, is it really Athena that’s being used to attest? HIMSS Analytics shows that most of Athena’s 25 sites are still running RazorInsights for registration, scheduling, and patient billing, so wouldn’t they also be running at least parts of the Razor clinical package, too?”
From Bushie: “Re: Athenahealth. Is it undervalued as the activist investor says?” Value is whatever the buyer thinks it is, but certainly the company has struggled to meet longstanding high-flying expectations as investors begin to question its slowed growth, management changes, forays into marginally related business lines that are defended by deeply entrenched competitors (inpatient), slowing post-HITECH EHR sales, and erratic investor guidance and resulting performance. I would also question, as I have from the day the company announced its IPO, if there’s too much of a Jonathan Bush cult of personality among fanboy equities analysts and whether Athenahealth is really a tech high-flyer vs. a boring business process outsourcer that just sends scanned paper to teams in India for manual entry. The stock price jumped after last week’s announcement that Elliott Management had acquired a 9.2 percent stake (and Wall Street firms predictably applied their impressive 20-20 hindsight to immediately upgrade their share price targets), but that’s probably more of a kneejerk reaction to the assumption that change is inevitable. Carving up the business into parts that are more valuable than the whole doesn’t seem likely and I don’t see opportunities to gain unmet synergy. I suspect the biggest fear out there is that JB will be pushed out and Athenahealth will be left as just another mature, sometimes struggling, not all that interesting industry player whose arc flattened out short of expectations. Quite a few EHR companies looked smart when the government was paying for EHRs in its $40 billion cash for clunkers program, but nearly all of them are scrambling frantically to pivot into population health, analytics, or revenue cycle to prop up their businesses that weren’t prepared for the inevitable scale-back required once the HITECH fired had been extinguished and doctors realized that the EHRs they hated pre-HITECH weren’t any more likable just because someone else (you and I) paid for them. I’ll turn to readers – is ATHN undervalued, what changes should it make, and what companies might like to buy some or all of it?
From Carry On: “Re: HIMSS. What are they paying Steve Lieber these days?” The newest IRS Form 990 I can find is for the fiscal year ending 6/30/15, when he made $1.1 million, a number that’s sure to swell dramatically this year as his retirement benefits are paid out. HIMSS paid more than $400K that year to Carla Smith, Norris Orms, John Hoyt, Jeremy Bonfini, and Alisa Ray. I would enjoy dissecting the HIMSS 2015 990 form if anyone has it – it’s apparently not online anywhere like the older ones.
From Lengua Taco: “Re: VIPs. I was surprised to read that hospitals treat VIPs differently.” You must never have worked in one. My first eye-opening experience was when, as a recent graduate turned hospital department head (unimpressively – it was a crappy, for-profit rural hospital) the awful second banana executive nearly lost his mind upon hearing that the mother of our big-money ophthalmologist was being admitted. He cleared all the rooms around hers, mobilized the dietary people to make special meals well beyond their culinary capabilities, and bossed around the nurses and techs to make sure they tiptoed about deferentially and didn’t screw up clinically (which as any hospital person knows actually makes mistakes more likely in replacing well-honed routines with new exceptions). In hospitals, everyone is treated the same in the ED, but once they are admitted and are found to have connections, money, or power, they are elevated from economy class to first (which, like the best table at McDonald’s, still isn’t that great). Wealthy, demanding local businesspeople and politicians don’t share semi-private rooms with the unwashed rest of us, nor do celebrities or Middle Eastern oil sheiks who might get their own entire floor. I doubt their clinical outcomes are any better, though, just their accommodations, a free pass to break hospital rules, and the endless middle management fawning over their magnificence.
HIStalk Announcements and Requests
Nearly 40 percent of poll respondents say the most important factor in reducing US healthcare costs is to move to a single-payer system that eliminates middlemen, with the next top choices being to control prices and increase emphasis on prevention. Frank provided a thoughtful response in saying that consumerism has worked well with cosmetic surgical procedures, won’t work as well with routine outpatient care and non-emergent elective procedures, and won’t work at all with care in emergencies, with the aged, and involving terminal illness, at least without societal upheaval. He adds that, unfortunately, most of the cost is involved in those areas where consumerism isn’t effective. He also warns that medical technology is advancing in providing expensive treatments for more Baby Boomer conditions. Cosmos says the best use of federal money is for public goods that have not not been addressed by the free market, such as disease prevention, promoting access to care and insurance, and rewarding physicians who do the right thing. Cash payer says treatment costs should be standardized to allow consumers to shop effectively.
New poll to your right or here: does your business card or email signature list a certification or fellowship credential? That issue comes up sometimes in HIStalk, where people complain that I don’t list their FHIMSS, FACHE, CHCIO, etc. My policy is that I list only academic degrees above the US bachelor’s level, with one exception — the non-US MBBS, which technically is a bachelor’s degree but is equivalent to the US MD. I also don’t list licensure, but it gets fuzzy where someone’s practice requires only a bachelor’s degree, such as a nurse, where I wouldn’t ordinarily list either the BS or the RN but there’s otherwise no good way to indicate that the person is a nurse. Sometimes I omit even graduate “degrees” that LinkedIn shows came from unaccredited (and sometimes hilariously phony) schools or that were honorary rather than earned, thus upsetting the folks who are anxious to flaunt a pointless credential in hopes nobody will notice the source.
Readers funded the DonorsChoose grant request of Mrs. A in California, who asked for a projector, document camera, USB camera, and laser printer for her middle school’s library, where she teaches math to 150 students. She reports, “The document camera and projector have improved the quality of my instruction. We will often show different strategies with different colors so that students understand that there is more than one way to solve a math problem. Lately, students have been going up and presenting their work under the doc cam, while other students ask them questions about their work. I also use the document camera and projector heavily for instruction. One particular student who has warmed to the doc cam and projector is Ramses. He loves presenting his work, and he was the first student to do so under the document camera in my 6th grade class. After he presented, students gave him ‘glows’ and ‘grows feedback about his presentation. Now other students present based on his model presentation and students are able to practice presenting their work proudly in front of their peers.”
This Week in Health IT History
One year ago:
Kansas Heart Hospital (KS) pays a hacker after a ransomware attack, but still doesn’t regain access to its systems.
Fired Practice Fusion founder and CEO Ryan Howard launches iBeat, which will offer a heart monitor and emergency notification watch.
Apple CEO Tim Cook says the company is focused on health and its entry point will be Apple Watch, which will have new sensors added.
HP announces plans to spin off its enterprise services business in a merger with CSC.
Paul Tang, MD joins IBM Watson Health as VP/chief health transformation officer.
Five years ago:
Cerner CEO Neal Patterson predicts that the company will hit $10 billion in annual revenue by 2020 and says he will probably retire before then.
Victoria, Australia ends its HealthSMART hospital software project that involves Cerner, CSC, and InterSystems after running over budget to $557 million.
HealthCor launches a proxy fight against Allscripts following the resignation of three Eclipsys-connected directors the previous month.
The VA announces plans to spend up to $5 billion to enhance VistA via the private sector and open source community.
US CTO Todd Park announces the Presidential Innovation Fellows Program.
The UK NHS announces plans to shut down its HealthSpace personal health record.
Weekly Anonymous Reader Question
I made last week’s question too specific, I think, given the small number of responses to the question of the most customer-unfriendly contract term or condition seen. I’ll just list those few responses here:
Charging maintenance fees for applications that just kicked off an implementation, as well as charging implementation and hosting fees! The ultimate double-dip rip-off.
Arrogant PeopleSoft VP refused to include any language protecting the customer should they be acquired, after all, “they are PeopleSoft”. Two years later, Oracle had them.
Non-compete clauses that inhibit people from their employment choices.
Having one vendor try to set the terms for who else I can engage with to optimize pieces of my organization. I have software I like to buy. And I have professionals I prefer to do business with for process improvements. When the software company tries to restrict my ability to engage with the professionals I trust, I view that as very unfriendly toward me.
Activist investor Elliott Management takes a 9.2 percent stake in Athenahealth.
Two highly-touted, well-funded, for-profit primary care clinic chains fail.
GQ exposes the efforts of fired Trump campaign manage Corey Lewandowski to sell access to the President, with Flow Health hiring the company hoping to reverse the VA’s termination of its data analysis contract.
Global impact of the WannaCry ransomware is muted when a security researcher finds and activates its kill switch.
Webinars
None scheduled soon. Previous webinars are on our YouTube channel. Contact Lorre for information on webinar services.
Decisions
Johnson Memorial Hospital (IN) will switch from Meditech to Cerner in August 2017.
Marshall Medical Center (CA) will replace McKesson with Epic in November 2017.
St Michaels Medical Center (NJ) went live with Epic this year.
These provider-reported updates are supplied by Definitive Healthcare, which offers a free trial of its powerful intelligence on hospitals, physicians, and healthcare providers.
People
Melissa Bell (MedAssets) joins Inovalon as SVP of client success.
Jim Feen is promoted to SVP/CIO at Southcoast Health (MA).
Announcements and Implementations
Messaging and patient engagement technology vendor Talksoft integrates its appointment reminder app with Uber, allowing patients to click an app button to call a car to take them to their appointment.
Teladoc will expand telemedicine services in Texas following the end of its six-year legal battle with the state over the now-eliminated requirement that patient-physician relationships begin with a face-to-face visit.
Other
Doctors at MUSC’s Medical University Hospital (SC) are reportedly “livid” that the hospital will start paying them based on the number of patients they see (RVUs) instead of based on the profits of their department. The CEO says that doctors who aren’t clinically productive “are going to have a tough time. Everyone has to be accountable to this clinical productivity.,” He adds that the current system is unfair to trauma surgeons who treat uninsured patients but benefits gastrointestinal surgeons who treat mostly Medicare patients. A patient safety advocate whose son died from a MUSC medical error says, “Paying doctors by RVUs is a terrible system and absolutely antithetical to patient safety, never mind workplace satisfaction. The doctors are right to be worried. I think this is a real comment on the priorities of the current MUSC leadership.”
Activist hedge fund operator Elliott Management takes a 9.2 percent position in Athenahealth, sending ATHN shares soaring 22 percent Thursday.
The fund issued its standard language that refers to “operational and strategic opportunities” (often involving selling the company) and expresses its interest in engaging with Athenahealth’s board.
Elliott has pressured other healthcare-related companies to increase shareholder value, most recently The Advisory Board Company and Cognizant.
Reader Comments
From Justin Box: “Re: Mary Washington’s video ‘Right Hand Man.’ We’ve reposted it on YouTube.” Justin, who is SVP/CIO of Mary Washington Healthcare (VA), said the hospital initially pulled the unlisted video from YouTube after I mentioned it Tuesday since it was intended to be for an internal audience only, but has since decided to repost the original, unedited version, which is spectacular. The hospital’s marketing people did an amazing job putting it together and the hospital employees who appear in it were fantastic. This would win my HISsies Best Picture award if I had one. Here’s an even more impressive factoid from Justin – President and CEO Mike McDermott, MD, MBA came up with the Hamilton theme idea, wrote the lyrics, and took on the starring role. I’ve watched it at least 10 times so far today. In one of those IMDB-type “goofs,” listen for the Epic product name that is mispronounced.
From Aftab: “Re: Aspen Valley Health (CO). A failed Epic implementation caused a loss of millions of dollars and the RIF of dozens of long-term employees. The 20-something IT director brought in an inexperienced team with no healthcare background and farmed out the technical IT jobs to an Indian outsourcing company. There was open revolt from the hospital staff, coupled with the CEO and CIO leaving.” Unverified. The 25-bed hospital signed up for Epic at a cost of $5.4 million in October 2015, affiliating with UCHealth. I reviewed the online video minutes of the hospital’s recent board meetings to look for updates — in the March 2017 session, the board talked about choosing a new EHR from among Cerner, EClinicalWorks, and current vendor Meditech, focusing on a system that is “affordable and accessible to any practice.” The board also wants its own MPI that isn’t shared with another hospital and its own EHR build. The board also noted that Cerner and EClinicalWorks are cloud-based, while Meditech would require 50 hospital servers, but they want to make sure cloud-based systems are ready for prime time. They’ve issued an RFI and hope to be live by 2020.
From Publius: “Re: Health Gorilla. Have you heard of them? They’re seemingly a Web-based EMR that supports electronic lab ordering. Is it used by smaller private practices?” I’ve mentioned the company a few times, labeling them as a “medical record aggregator” and secure network that allows sharing records and placing electronic lab orders. Practice price ranges from free to $60 per month. The Silicon Valley-based company – formerly known as Informedika — has raised $4.4 million, none of it recently, and hasn’t issued a press release since October 2015.
From SugerHound: “Re: Apple Watch and glucose monitoring. The rumors are more substantial than are being reported. Chrissy Farr has a great report on CNBC that cites multiple sources.” The article says Apple’s team of biomedical engineers has been developing non-invasive blood glucose sensors for several years in a project originally envisioned by Steve Jobs. They are reportedly conducting feasibility trials and figuring out how to earn FDA approval, which probably won’t come easily or quickly.
HIStalk Announcements and Requests
Readers funded the DonorsChoose grant request of Ms. S in California, who asked for non-fiction books for her third graders, with an emphasis on the environment. She reports, “My students and I have become passionate about plants! Not just any plants, but native plants in particular. The chaparral biome which surrounds our school and community is thriving with plant and animal life. Using the books that you so generously donated, my students learned about the environment, and they started a close study of their backyard ecosystem: the chaparral. Caring for the plants and becoming experts of many of the living things in our ecosystem, my students are now serving as stewards for the environment. Without your generous donation, our project would not have been able to take off.”
My “Listening” selection from three weeks ago was the new solo release of Soundgarden and Audioslave front man Chris Cornell. He died by suicide Wednesday night after a Detroit performance of the reunited Soundgarden. His last song on stage was a cover of Led Zeppelin’s “In My Time of Dying.”
This week on HIStalk Practice: One Medical opens first practice in Seattle. Vivid Vision raises $2.2 million for VR-enabled vision disorder treatment technology. US HealthWorks develops telemedicine app. MD EMR Systems, Bridge Patient Portal work on Centricity integration. CMS allocates $30 million for medical societies interested in helping to develop MACRA measures, adds four regions to CPC+ program. Premise Health will roll out Epic over the next two years.
Webinars
None scheduled soon. Previous webinars are on our YouTube channel. Contact Lorre for information on webinar services.
Acquisitions, Funding, Business, and Stock
A Singapore-based private equity firm buys a majority position in supply chain technology vendor Global Healthcare Exchange from PE firm Thoma Bravo, which bought the business in February 2014 and will remain a minority owner.
Seattle-based primary care clinic Qliance Medical Management, which had raised $33 million from investors that included Amazon’s Jeff Bezos, shuts down. The two principal officers bought the company in March 2016 from its investors.
Clinical process improvement technology vendor LogicStream Health closes a $6 million Series B funding round.
Credentialing and compliance software vendor Symplr acquires Vistar Technologies, which offers a provider data management system.
Conversa, which offers doctor-patient conversation programs, raises $8 million in a Series A funding round led by the venture arm of Northwell Health (NY), which will also use the company’s systems.
UnitedHealthcare subsidiary Harken Health, launched in 2015 to offer health insurance combined with low co-pay visits in its Atlanta and Chicago health clinics, will shut down after extensive losses.
Amazon is considering entering the pharmacy market, according to reports, which could involve either selling drugs online (which it already does in Japan) or extending its in-house pharmacy benefits management program.
McKesson is basically out of the health IT business (or will be soon), but if anyone still cares, the company announces Q4 results: revenue up 5 percent, EPS $16.76 vs. $1.88, although that includes a pre-tax net gain of $3.9 billion related to the creation of Change Healthcare. MCK shares rose 6 percent in early after-hours trading Thursday, having beaten earnings expectations but falling short on revenue.
Sales
National non-profit behavioral health provider Compass Health Network chooses Netsmart’s EHR in a 10-year agreement.
The VA awards Document Storage Systems (DSS) a $19.6 million contract to implement its ForSite2020 patient self-scheduling system that integrates with VistA. DSS acquired the product in December 2016 with its $2 million purchase of Streamline Health’s Looking Glass patient scheduling and surgery management software, which Streamline had previously bought in its February 2014 acquisition of Unibased Systems Architecture.
Prime Healthcare will implement real-time sepsis surveillance systems from Hiteks Solutions, integrated with Meditech and Epic.
People
Robert Califf, MD — who served less than a year as FDA commissioner before the administration change — returns to Duke Health as vice chancellor for health data science and will also split time in a leadership role at Alphabet’s Verily Life Sciences, where he will work with turning health-related data into practical applications. Verily, formerly known as Google Life Sciences, has worked on continuous glucose monitors, smart contact lens, retinal imaging, and surgical robotics.
Announcements and Implementations
Visage Imaging releases its Visage 7 Open Archive solution of its enterprise imaging platform to customers in North America.
Athenahealth announces a Meaningful Use Stage 3 guarantee for its hospital customers. The company also opens San Francisco-based MDP Labs, an innovation program that offers workspace, mentorship, and exposure to potential investors, partners, and customers.
Healthgrades enhances its online scheduling system to allow health systems to display their nearby alternative providers when a given one is booked up.
Siemens Healthineers will integrate test results from its HbA1C and urinalysis diagnostic equipment with practice-based EHRs via technology from Scotland-based Relaymed, owned by Goodmark Medical of Longwood, FL.
CHIME announces the finalists in its patient ID technology challenge that will move to the prototype testing round:
Michael Braithwaite (multiple biometrics)
Bon Sy (behavior information, biometrics)
HarmonIQ Health Systems (blockchain, FHIR, encryption)
RightPatient (photos, biometrics, other data)
Government and Politics
The Justice Department files a civil fraud lawsuit against UnitedHealth Group, claiming that the insurer was overpaid at least $1 billion in Medicare Advantage payments after intentionally submitting inaccurate risk adjustment data. UHG says it tried to comply with CMS’s “unclear policies” and adds that the Justice Department either misunderstands or ignores how Medicare Advantage works.
Insurance company executives and state insurance regulators say the ACA insurance marketplaces aren’t collapsing under their own weight, but rather because of the Trump administration’s erratic management, vocal lack of support, and ongoing threats to stop payments, according to an LA Times article. In a remarkably partisan response for a federal department employee, 28-year-old Alleigh Marre — quoted as an HHS spokesperson but self-identified on her LinkedIn profile as a “Republican Communicator,” — said, “Obamacare has failed. For this reason, Republicans are reforming healthcare so it delivers access to quality, affordable coverage to the American people.” The article also notes that CMS Administrator Seema Verma told insurance company executives that the White House would continue allowing the payment of cost-sharing reductions (premium subsidies, required by law to be paid unless a court rules otherwise) if insurance companies would in turn support the Republican ACA repeal bill, a puzzling offer (even for a near-shakedown political demand) since repeal would do away with the subsidies.
Privacy and Security
Bronx-Lebanon Hospital Center (NY) and its contractor iHealth send threatening cease-and-desist letters to the author of DataBreaches.net after she let the hospital know that their patient information was exposed due to an improperly configured server, for which the hospital originally thanked her. They claim that the discovery of their apparent screw-up constitutes “hacking,” which happens often when companies are embarrassed and attempt to shoot the messenger.
Erie County Medical Center (NY) finally confirms that the April 9 cyberattack from which it is still recovering six weeks later was indeed ransomware, which had been widely speculated. The hospital declined to pay and was forced to move back to paper as its systems were slowly brought back online from backups. They don’t believe it was the WannaCry malware.
Technology
Google is applying machine learning to millions of de-identified patient records from major teaching hospitals to see if it can predict an individual’s medical events.
Google’s major announcements from its developer conference:
Google Lens, an app that can identify objects from a smartphone’s camera.
New Daydream virtual reality headsets.
Photo facial recognition that will suggest sharing images with people pictured in them and AI-powered removal of unwanted objects in photos.
A visual positioning system that will identify a precise location based on nearby objects, such as finding items on a store shelf.
The addition of calling and proactive information presentation to Google Home and the porting of Assistant to the iPhone.
In India, Aetna rolls out the first phase of its global launch of it subscription-based vHealth by Aetna, which offers unlimited PCP visits by video or telephone, diagnostic tests at home, home prescription delivery, and referrals. Patients can rate their doctor experience afterward.
FiercePharma profiles Israel-based MedAware, which uses aggregated prescription data and a patient’s own medical records to predict what drugs are likely to be ordered, improving patient safety in providing what it calls a “spell checker” for prescriptions. The CEO has astutely noted that all of that information is also attractive to drug companies that are interested in targeting their physician prospects, giving it an unexpected yet lucrative market.
Other
Boston Children’s Chief Innovation Officer John Brownstein weighs in on the language in Epic’s App Orchard agreement, which basically says that Epic can use any of the submitter’s information to develop a competing product and that Epic permanently owns any documentation that the applicant submits. In other words, it’s exactly opposite of the highly restrictive language contained in Epic’s customer contracts.
In an interesting twist on medical tourism, a nearly completed medical center in Jamaica plans to lure not only medical tourists to fly there for procedures at discounts of up to 40 percent, but also to recruit American doctors to perform the work while taking a Caribbean vacation. Critics point out that it’s been tried before, failing because doctors are too busy to interrupt their vacations and are not likely covered by their malpractice insurance when doing work outside the country.
Bizarre: Michigan suspends a DO’s license after a patient complained that her liposuction surgery was performed in an unfinished pole barn, during which the doctor poured her removed fat down a sink drain.
Sponsor Updates
Medicity and Clinical Computer Systems, developer of the Obix Perinatal Data System, will exhibit at the Texas Regional HIMSS Conference May 25 in San Antonio.
Wavelink is named as the first Spok distributor in Australia.
Medecision presents its annual innovation awards at its Liberation 2017 conference in Austin, TX.
Definitive Healthcare is recognized by Boston Business Journal for its growth and work environment.
FormFast and Imprivata will exhibit at the 2017 Spring Hospital & Healthcare IT Conference May 22-24 in Atlanta.
GQ publishes an article critical of fired Donald Trump campaign manager Corey Lewandowski, who tried to parlay his connections to the President after his June 2016 dismissal into a lucrative lobbying business that includes a health IT connection.
Among the clients Lewandoski recruited was Flow Health (the former GroupMD), which hired Lewandowski’s firm in December 2016 to pressure the VA to reconsider its termination of Flow Health’s contract for AI-powered patient care systems.
GQ reports that Lewandowski’s partner (who managed Ben Carson’s presidential campaign) told Flow Health CEO Alex Meshkin that the lobbying firm could reverse the VA’s decision because he and Lewandowski were personally vetting Trump’s picks for VA secretary. He also promised that the firm would allow Flow Health’s CEO to submit a list of his preferred choices for role of VA CIO, overseer of the Flow Health decision.
The article says that Flow Health proposed an apparently illegal payment schedule of a flat payment of $250,000 if the VA reversed its decision by February 17 and $100,000 if it took an extra week, later amended to reword the payments as severance fees. None of that mattered, as it turned out, because Trump chose as VA secretary David Shulkin, who had co-written the letter that dismissed Flow Health in the first place.
GQ says Lewandowski then proposed that Flow Health do an end-run around the VA by either appealing to Trump directly or by using Lewandowski’s appearance on the Sean Hannity talk show to trash Shulkin in hopes of getting him fired.
Lewandowski quit the firm – for which he was serving as an unregistered lobbyist — two weeks ago after widespread questions about his efforts to sell access to the President, which he calls “fake news” and for which he blames his former partner. Flow Health’s VA contract remains terminated.
Googling “Alex Meshkin” turns up a fascinating Bloomberg story from 2005 about the then-24-year-old’s questionable background as he formed a Nascar racing team that quickly failed.
Reader Comments
From Athenahealth Spokesperson: “Re: Diego’s questions about Athenahealth’s inpatient customer MU attestations. All 35 hospitals referenced are using Athenahealth’s complete inpatient solution, including EHR, revenue cycle and financial management, care coordination, and patient engagement services. This past year, Athenahealth submitted Meaningful Use attestations on behalf of all of our hospital clients live on AthenaClinicals for Hospitals & Health Systems as of the end of 2016.”
From Cerner Observer: “Re: Mon Health, Morgantown, WV. Hearing that its Cerner go-live has been pushed back to 2019 and they’re exploring other options.” Unverified. I couldn’t find a contact there to ask for verification. I was, however, a bit annoyed to observe that the locals are so challenged to pronounce the name of the county in which they live (Monongalia) that the health system that lives in the shadow of Epic-using WVU Medicine felt the need to officially dumb down its name to “Mon Health,” giving me visions of those rainbow-colored (and uncomfortably stereotypical) Rastafarian dreadlock hats you see for sale on vacation in the Caribbean that say “Hey, Mon, we be jammin!”
From Second Responder: “Re: anniversary date. Isn’t HIStalk’s anniversary coming up soon? I remember it’s late spring.” I started writing HIStalk in June 2003, although I don’t recall the exact date.
From Judith R. Lin-Miranda: “Re: video. It’s now a common practice for new Epic customers to introduce themselves. Mary Washington Health Care just set the standard by which all others will be judged.”The elaborate video is indeed well done, including taking some digs at Siemens/Cerner Soarian that was “cobbled together” as they were “working with a third of what Soarian promised.” The video even lobs some shots at Epic’s high cost. President and CEO Mike McDermott, MD, MBA did an amazing job in the lead role. It’s better than anything ZDoggMD has done. I would give it my “Best Picture” award if I had one.
From Gory Details: “Re: press release. Here’s ours, which you probably won’t mention since we aren’t an HIStalk sponsor.” Not true. I mention every press release that I think is newsworthy to my C-level audience, which typically includes all sales and go-lives that: (a) involve a vendor, client, and event that are all significant; (b) would interest readers who don’t follow the company; and (c) contain a link to a timely press release that is well enough written that I can quickly figure out what it’s trying to say. Otherwise, readers outside the company usually aren’t interested in fluff pieces about partnerships, self-proclaimed market momentum, and minor personnel and funding events and I’ll nearly always skip those. I’ve learned over the years that every company executive thinks all of their announcements are anxiously awaited, which is nearly always not the case. Do something newsworthy and you’ll see it on this page.
HIStalk Announcements and Requests
HIStalk readers funded the DonorsChoose grant request of Ms. W, who asked for tablets and headphones for her California kindergarten class to extend their environmental studies. She reports, “The Fire tablets have been such a great learning resource for my students. They love using them to watch ‘Meet the Environmental Defenders.’ They love singing along to the song. You can hear them chanting quietly, ‘Reduce, reuse, recycle!’ They do this over and over again. Next thing you know, that tune is stuck in my head all day long!”
I’ve noticed a recent sneaky practice of call centers (both inbound and outbound) that place you on hold, but play pre-recorded keyboard clicking sounds so you think a human is on the line.
A reader offers a third punk band whose singer has a PhD (in addition to those I named, Bad Religion and The Offspring): The Descendents, which has been a major influence to untold bands that aren’t even punk for its 40 years of existence. Milo Aukerman left the band to complete his PhD in biology at UCSD and conducted post-doctoral research in biochemistry at UW-Madison. His nerdy caricature is the band’s mascot, rolled out in 1982 for the album “Milo Goes to College” that noted his temporary departure. Beyond all that academic talk, there’s a new hard-rocking album from Seether that’s worth a listen.
Webinars
None scheduled soon. Previous webinars are on our YouTube channel. Contact Lorre for information on webinar services.
I asked John Gomez to put together a WannaCry malware webinar with only hours of lead time because his presentations are always outstanding and informative. This one he did Tuesday afternoon is no exception. I was attentive for the whole thing, which isn’t usual for me since I have a short attention span. Thanks to John for agreeing to help get information out quickly.
Acquisitions, Funding, Business, and Stock
Wisconsin startup IDAvatars, which develops healthcare avatars powered by IBM Watson, opens a funding round in hopes of raising $2 million.
Sales
Premise Health will implement Epic in its 500 work site health and wellness centers. It apparently replaces Greenway Health.
University of Miami Health System (FL) chooses Kyruus Provider Match and KyruusOne to connect patients with providers based on their clinical needs and preferences.
The Commonwealth of Virginia and Bayview Physicians Group will integrate Appriss Health’s prescription drug monitoring program analytics software into provider EHR workflow.
People
Mark Costanza (Nordic) joins Spok as SVP of professional services.
Announcements and Implementations
Memorial Hermann Memorial City Medical Center (TX) goes live with a digital wayfinding app powered by Connexient’s MediNav.
National Decision Support Company adds appropriate use criteria for pediatric imaging to its ACR Select product.
CPSI’s TruBridge subsidiary announces its business intelligence dashboard at the company’s user conference.
Government and Politics
Social media outcry pressures Miss USA to walk back her comments from the Q&A portion of the competition in which she stated that healthcare is a privilege rather than a right, unconvincingly explaining that what she really meant is that she is “privileged” to have healthcare, but regardless, it’s a “right” for all.
Missouri’s lost its chance to stop being the only state that doesn’t have a doctor-shopper prescription database as legislation to authorize it failed Friday after the Senate added a mandatory prescriber participation clause, which was opposed by the state medical association.
Privacy and Security
HHS says in a ransomware update call that several medical devices have been infected with the WannaCry virus, but otherwise the US healthcare system seems mostly unaffected for now. Several hospitals around the world reported that they were attacked. Northwell Health (NY) initiated its incident command system Friday morning and patched 200 computers that were behind on Microsoft security updates.
In England, a leaked February letter from National Data Guardian Dame Fiona Caldicott to Royal Free Hospital’s medical director says the hospital should not have turned over the detailed records of 1.6 million patients to Google DeepMind for testing of its Streams application, saying it was not appropriate to send Google the information without patient permission since it was not related to their care.
Rutland Regional Medical Center (VT) becomes the latest in a long string of hospitals that have exposed patient information by sending a bulk email to patients using CC: instead of BCC:.
Marcus Hutchins — the 22-year-old security researcher who interrupted his vacation to stop the global spread of the WannaCry virus by discovering and activating its kill switch before it hit US hospitals – is awarded a $10,000 hacker’s bounty that he will donate to charities. He works from a spare bedroom in his house in England for US-based Kryptos Logic.
Other
Wired runs a lengthy piece describing the last creation of Steve Jobs, Apple’s $5 billion, 2.8 million square foot mother ship campus.
A graphic, moving blog post by ED physician Kristen Ott, MD explains that medical professionals use profane language outside of public spaces because they have to deal with the aftereffects of unspeakable atrocities that can’t really be described politely.
This should ring the cash registers of pharma lobbyists: three members of Congress introduce the Fair Drug Pricing Act, which would require drug companies to provide detailed cost and price records to HHS before increasing an expensive drug’s price more than 10 percent in one year or 25 percent over three years.
Australia-based surgeon Eric Levi, MBBS muses on the suicide of a Brisbane gastroenterologist, which triggered him to think about what factors lead him to his own “dark seasons” as a doctor:
Loss of control with extensive hospital call time and new physician-directed policies written by people who don’t see patients.
The impersonality of computer-assigned work, pressure to beat the timer that says tonsillectomies should take no more than 14 minutes of surgeon time, overbooked clinics, and never-ending telephone calls, all of which leave no time to reflect about life with colleagues or to spend time with friends and family. Doctors who ask for emotional support can be placed on restriction or labeled as underperforming.
Relentless administrative pressure that takes away meaningful patient engagement as medical practice transforms from a “meaningful pursuit” to a “tiresome industry” that has been “codified, sterilized, protocolized, industrialized, and regimented.”
Sponsor Updates
Point-of-Care Partners publishes a white paper titled “EPrescribing Information to Improve Medication Adherence.”
Arcadia Healthcare Solutions will speak at the HFMA Region 1 annual conference May 23 in Uncasville, CT.
CapsuleTech will exhibit at the National Teaching Institute & Critical Care Exposition May 21-25 in Houston.
Besler Consulting will exhibit at the HFMA Region 1 annual conference May 23 in Uncasville, CT.
CoverMyMeds will exhibit at the QS/1 Customer Conference May 17-19 in Atlanta.
Besler Consulting releases a new podcast, “Evaluating post-discharge cost and quality.”
CTG announces expanded portfolio management and help desk services in its Application Advantage program.
Cumberland Consulting Group will sponsor the ASO Opportunities Value Visit May 17-19 in Chicago.
Impact Advisors VP Lydon Neumann is named one of Consulting Magazine’s Top 25 Consultants of 2017.
The local business paper profiles Diameter Health and its ties to Connecticut Innovations.
May 15, 2017NewsComments Off on WannaCry Ransomware Webinar Tuesday, May 16
Sensato CEO and cybersecurity reseaercher John Gomez will present an HIStalk-sponsored free webinar on Tuesday, May 16 at 1:00 p.m. ET titled “WannaCry Threat Intelligence Briefing.”
John will provide an in-depth analysis of the current state of WannaCry as well as a technical review of how it operates and possible go-forward cybersecurity impacts. John will also present technical and regulatory counter-measures you should consider, specific to healthcare organizations.
An unprecedented ransomware attack affects 48 of England’s 248 trusts in waves of infections that spread globally on Friday. All but six trusts say they have returned to normal operations after they were forced to divert ambulances, cancel appointments, revert to paper, and order employees to unplug network cables from PCs and telephones.
The WannaCry ransomware, which demands a $300 ransom per infected Windows machine, initially affected computers primarily in Russia, Ukraine, and Taiwan. It uses the EternalBlue exploit that was made publicly available by hackers in mid-April. At least one hospital in Canada said it was threatened by WannaCry, but its antivirus software blocked it. Two hospitals in Indonesia were also hit as well as one in Taiwan and another in Scotland.
Microsoft issued a Windows patch to protect against the exploit in March, but many machines worldwide have not been updated. NHS is still running many Windows XP PCs, for which Microsoft’s extended support and security updates ended in 2014. Microsoft has responded to the attacks by providing an unprecedented public security update for Windows XP, Windows 8, and Windows Server 2003 to address WannaCry. Both Kaspersky and Bitdefender antivirus programs already protected against it.
The Russia-based hacker group that claims responsibility for the attack says it used cyber tools that were stolen from the US National Security Agency.
A 22-year-old security researcher apparently stopped the worldwide spread of WannaCry when his tests revealed that the malware was accessing an unregistered Internet domain, which he then registered to perform further testing. In doing so, he found that the ransomware stopped activating itself around the globe. The researcher theorizes that the hackers used the domain as a “kill switch” to prevent experts from analyzing in a sandbox environment. However, he cautions that the hackers could simply change the domain name the program checks, making it imperative that Windows PCs be brought up to date on patches.
A PC can be infected via a hyperlink spread by a phishing email, a web link or advertisement, or a document link.
John Gomez of Sensato offers these tips for health systems:
Apply the SMB patch (MS17-010) to all Microsoft systems.
Close ports 22, 23, 3389, TCP 139 and 145/UDP 137 and 138.
Test backups and store them offline.
Warn users not to open attachments.
Restrict access to file-sharing sites.
Review ransomware response protocols.
HIStalk Announcements and Requests
Eighty percent of poll respondents are not happy that the House passed the American Health Care Act. Frustrated says people should actually read the bill instead of parroting the opinions of others, adding that no healthcare system can survive if only sick people sign up and both the ACA and AHCA address that. Just a Nurse Analyst wonders about the backroom deals that were struck to pass it and questions the zeal to undo anything President Obama did regardless of the impact on Americans. Cosmos says every step of the process lacked moral discipline and integrity – the headlong rush and repeated attempts to repeat the ACA, the backroom negotiations, voting without CBO analysis, and a two-vote majority that suggests compromises undeserving of the resulting White House victory party. Malvern says that our healthcare cost of $10,000 per person each year can’t be solved by attacking coverage and premiums alone. Disgusted says it’s the most cynical, heartless pieces of legislation ever, especially the Medicaid cuts and the requirement of continuous coverage to have pre-existing conditions accepted. Printgeek thinks it’s a shame that the two political parties can’t even initiate a dialogue about healthcare. Bill says at least AHCA eliminates the word “affordable” as Congress finances access by increasing the federal deficit. HITgeek says healthcare requires a community health insurance risk pool to spread the cost of involuntary events, adding, “I am sick and tired of compassionless insurance, abetted by politics, being the gatekeeper for US healthcare.”
New poll to your right or here: What’s the most important factor in reducing US healthcare costs? The presence of the word “most” means I’m not oblivious to the desirability of an easy-out “all of the above” response, although I provided an “other” box in case my mental checklist of options is incomplete.
We funded the DonorsChoose grant request of Ms. L in Michigan, who asked for Chromebooks, headphones, and academic software subscriptions for her fourth grade class. She reports, “I am a fourth grade teacher on paper, but in reality, I teach students anywhere from a first grade to a fourth grade level. This poses a very real challenge that both my students and I deal with head-on. Technology is one way to successfully mitigate this particular hardship and thanks to you, our class was able to get the technology we need to be successful! Students have grown tremendously through these online platforms; we track and celebrate their progress weekly! It also makes students feel that they are valued. They have something BRAND NEW, that people whom they will never meet gave to them. That sense of value and feeling appreciated is HUGE and cannot be overstated. Thank you, thank you, thank you for making our class feel important!”
This Week in Health IT History
One year ago:
Theranos says 2014-2015 lab test results from samples it ran using its proprietary Edison analyzer should not be trusted.
The VA releases a software development kit for its open source Enterprise Health Management Platform.
Competing Missouri HIEs argue over connectivity, member charges, and unnamed special interests.
Five years ago:
Partners HealthCare announces plans to implement Epic at a cost of $600 million.
Greenway Medical Technologies is the largest percentage gainer on the New York Stock Exchange, with shares up 20 percent since the company’s February IPO.
NextGen parent Quality Systems acquires EDIS vendor The Poseidon Group.
3M makes its Healthcare Data Dictionary available worldwide at no cost.
California’s HHS moves oversight of the Cal eConnect HIE to the Institute for Population Health Improvement.
Allscripts appoints Paul Black to its board.
A report finds that one-third of prescriptions are being sent electronically.
Fairview Health Services admits that it was getting extensive negative feedback from its employees about the strong-arm collection tactics of Accretive Health.
Weekly Anonymous Reader Question
I’m delighted that my anonymous reader question surveys are getting so many responses that they don’t fit nicely into the Monday Morning Update. I’ve posted the two most recent sets of results at these links:
This week’s survey: What is the most customer-unfriendly term or condition you’ve seen in a healthcare software contract that the customer approved? This would be a good opportunity to warn others about items they shouldn’t accept.
Meanwhile, if you have ideas for future surveys, let me know – it’s an easy way to learn what your peers are seeing or thinking.
Last Week’s Most Interesting News
ONC appoints Genevieve Morris, MA (Audacious Inquiry) to Principal Deputy National Coordinator for Health Information Technology.
Memorial Hermann Health System (TX) pays $2.4 million to settle HIPAA charges after naming an arrested patient in a press release.
Specialty EHR vendor Modernizing Medicine raises $231 million in funding.
A contractor’s error exposes patient records of Bronx-Lebanon Hospital Center (NY) to the Internet due to a misconfigured backup.
Webinars
None scheduled soon. Previous webinars are on our YouTube channel. Contact Lorre for information on webinar services.
Acquisitions, Funding, Business, and Stock
Google parent Alphabet invests $130 million in San Francisco insurance startup Clover Health, raising its total to $425 million and valuing the company at more than $1 billion. Clover manages claims for just 25,000 Medicare Advantage customers in New Jersey and competes against much larger insurers, but says its forte is mining patient data to identify potential problems that can be addressed via a Clover-managed home visit or other intervention.
Decisions
Memorial Hospital of Lafayette County (WI) will switch from Medhost to Epic in November 2017.
Kaweah Delta Health Care District (CA) will replace Cerner/Siemens Soarian with Cerner Millenium in November 2017.
Haxtun Hospital District (CO) switched from NextGen Healthcare to Athenahealth in April 2017.
Platte Valley Medical Center (CO) will go live with Infor human resources in May 2017.
These provider-reported updates are supplied by Definitive Healthcare, which offers a free trial of its powerful intelligence on hospitals, physicians, and healthcare providers.
People
Allscripts promotes Dennis Olis to interim CFO following the resignation of Melinda Whittington, who is leaving the company for unstated reasons after just over a year on the job .
Government and Politics
MedSolutions CareCore – now part of specialty benefits manager EviCore — will pay $54 million to settle an HHS fraud lawsuit in which the company authorized Medicare and Medicaid payments for procedures it had not validated as medically necessary. The company admits that its executives monitored a dashboard of medical review cases, and when the list got too long, ordered clinical reviewers to approve requests for prior authorization even though nothing had changed, which the Department of Justice says resulted in improper payment in up to 300,000 cases. EviCore was rumored earlier this month to be reviewing a sale of the company or an IPO, with its $300 million in 12-month EBITDA valuing it at up to $4 billion.
A former podiatrist pleads guilty to defrauding Medicare of $6 million by implementing an EHR in his 16-state long-term care practice to generate false patient documentation that would earn payments, such as falsely describing toenail conditions as “painful to such a degree as to affect ambulation and balance.”
Privacy and Security
The local paper reports that Erie County Medical Center (NY) is still trying to recover its systems more than a month after an apparent ransomware attack.
Other
The New York Times questions advertising drugs directly to consumers – legal in only two countries, the US and New Zealand — in noting TV commercials for a drug for an uncommon neurological condition for which it can stop uncontrolled crying or laughing. It notes that the commercial will likely pique the interest of overly emotional people well outside the drug’s target market who will pester their doctors to prescribe them the $700 per month drug.
Interesting: Dexter Holland – singer/songwriter of punk rock band The Offspring for more than 30 years – earns his PhD in molecular biology from USC with his dissertation titled “Discovery of Mature MicroRNA Sequences within the Protein-Coding Regions of Global HIV-1 Genomes: Predictions of Novel Mechanisms for Viral Infection and Pathogenicity.” As a clearly Renaissance man, he also has his own brand of hot sauce, is the former owner of a record label, and is a certified flight instructor who made a solo trip around the world in 10 days. Dr. Holland isn’t the first punk rocker to earn a PhD – Bad Religion founder Greg Graffin earned a Cornell doctorate in zoology and has taught and written on academic topics.
In Canada, Island Health tells nine internists who are refusing to use its Cerner-powered EHR because of patient safety concerns that they will no longer provide other doctors to enter their paper orders electronically. The CEO of Island Health says it’s OK that ED and ICU doctors haven’t used the systems – citing similar concerns – because they never fully transitioned to the EHR, but it’s too late for the internists to go back to paper. One of the protesting doctors, who is also president of the hospital’s medical staff, says the decree puts him in a difficult position because “it has the effect of barring me from practicing … without actually suspending me.”
Weird News Andy says that even though Sir Winston does not approve, he suggests ICD S01.22XS. In England, cocaine users are “getting Winstoned” when they use new, stiffer five-pound bank notes bearing the image of Winston Churchill to snort their drug of choice, leaving them with nose cuts.
Sponsor Updates
Gartner names Salesforce a leader for the ninth consecutive year in its Magic Quadrant for the CRM Customer Engagement Center.
The SSI Group will exhibit at the HFMA Spring Joint Conference May 17 in St. Louis.
TierPoint will host a grand opening for its Dallas-Allen data center on May 18 in Allen, TX.
The Chartis Group publishes a white paper titled “The Impact of the American Health Care Act on Children’s Hospitals: Preparing for the Road Ahead.”
TransUnion publishes a new white paper, “Uncompensated Care is on the Rise.”
Conduent reports first quarter 2017 financial results.
ZirMed publishes a new infographic, “ZirMed Denials by the Numbers.”
At a CIO’s request, I asked former and current CHIME members who have either quit or thought it to explain why.
I was once a CIO member years ago. Great networking and exchange of ideas. I became vendor, and after several years, pulled out. It became a pay-to-play with diminishing value. Let me tell you, even the sponsor companies don’t like it much.
It’s become a mini-me of HIMSS.
Vendors are running the show and there is no sense of working to better the industry.
CHIMe used to be an exclusive group of of IT executives and limited number of foundation members (vendors and consultants). Now it’s a mini-HIMSS dominated by vendors, with limited value for all participants. I’m not sure what CHIME’s mission is any more.
Way more time spent with the Foundation members than with fellow CIOs.
It has become so vendor-heavy and the membership drive now allows most anyone to join.
As a CHIME Foundation member for 12 years, I am disgusted with the direction both CHIME and HIMSS are going. It has become a”Russ Branzell “let’s look as much like HIMSS as we can” show. Quantity is more important than being a true CIO venue, having invited people as far down as the director level. I talk to a lot of CIOs who are no longer attending CHIME because of their new focus on money rather than collaboration. As a vendor, I no longer get the same value and am paying a lot more money for decreased value. I still feel I have to belong, just like HIMSS, because absence in noted more than presence.
Just like HIMSS, all about collecting vendor money and less about colleagues teaching and learning from each other. It is overwhelming being a CIO and have to deal with eight vendor staff to each one of us.
As long as CHIME works to keep the vendor contacts at the highest executive levels (Carl, Judy, etc.) it is fine. Complete openness and transparency is needed to give confidence that it exists to serve its members and not enrich its leaders though lucrative associations and spin-off ventures.
I’ve been involved in HIMSS and CHIME for many years, but have limited participation due to the vendor involvement. This has changed the focus for both organizations from members to vendors.
The move away from being a CIO-focused organization to having a variety of members, especially vendor firms.
It has taken on the same mentality as HIMSS — expand the focus to more vendors and non-CIO types. I attended HIMSS for the education sessions and the focus moved away from them. I attended CHIME for networking and CIO sessions to learn what others were doing. Sorry to say this has grown so much it does not work any more. It does not matter to me anyway because I have retired. There is a group of CIOs that formed HISEA. I could not join because a competitor CIO was already a member and that rules out many. But the concept was centered on presentations of great new ideas for other CIOs.
They are selling access to us. It felt a bit more subtle in the past, but is not that way and feels far more commercial.
I don’t like the Fall Forum. Too many vendors, the focus groups are a waste. It is clearly a business, not a professional society. Too bad.
Seeing declining value from participation year to year.
I was booted from CHIME after being a long-time member because I became employed by a healthcare vendor instead of a healthcare provider. I understand the rules, but there are plenty of old timers who are still members even after they went to work on the vendor side because their company has the massive funds to become a CHIME foundation member. So two reasons why I wouldn’t rejoin CHIME even it they would let me: 1) CHIME negates your years of healthcare provider experience once you go to work for a vendor, and 2) they purposefully exclude many vendors from the foundation by charging a huge amount of money for that privilege. I think that CHIME has done great work in the past, but I hate to see it become so commercialized and HIMSS-like.
The leadership seems more committed to growing members and expanding rather than serving the needs of the current membership.
Not providing value.
Insufficient value from membership.
I am considering it. The Fall Forum was the highlight of the year for networking with fellow CIOs and the Foundation firms. The last event I went to, the experience had dramatically changed. Now vendors have booths and instead of one or two people from a Foundation firm, there are MANY. Likewise on the CIO side. There are associate members that may number greater than the number of actual CIOs in attendance. This has moved from a very effective, intimate industry leader gathering to a mini-HIMSS. And who needs that? CHIME is clearly focused on growing revenue, just like HIMSS. I hope HIMSS selects a new leader that can actually save HIMSS from itself and that CHIME leadership watches closely and learns.
I asked readers: what specific event crystallized your decision to leave your last job?
I was asked if I’d be willing to relocate after 3 years at one office. Said yes so my manager started the process. He never even told me what the HR package was, as it was so insulting. Knew then that it was time to leave the (slowly) sinking ship.
The PE firm that bought our company had little interest in the actual work we were doing. The CEO they put in place fell asleep in the first customer meeting I took him to and then after the meeting told me the customers in the meeting were idiots and he would rather get a needle stuck in his eye than attend another meeting like that.
Was notified by McKesson in fall 2016 my job would end March 31, 2017. Two months later was told I would need to train offshore resources how to utilize and quality test a large piece of clinical software. Given my training and years of front line experience in hospitals, my principles were on the line and no amount of severance was going to compensate me for principles. I turned in my two-week notice in early 2017 with several irons in the fire, but no offers. On my last day at McKesson, I got a call at noon offering me the job I was hoping for.
I took an early retirement package equaling a year’s pay, easing the way into lucrative consultancy for the next few years. However, the event that crystallized my decision was the concurrent layoff of valued colleagues who did not qualify for the package. It was the right choice.
To start a new company and see an idea turned into reality. Hopefully, hah.
Micromanaging leadership and leaders out for self-promotion over the company’s goals.
I was working 60-70 hours per week, seven days a week. My boss assigned me another project, and when I told him I couldn’t, he said something about digging deeper and that I could do just a little more. I already knew I was going to quit, but was trying to hold off one more month. That sealed me. They distributed my work among nine people.
I was a founding but minority partner in a consulting firm. After Having several disagreements with our managing partner about the future direction of the firm, I reached out to our board chair for advice. He made it clear that the managing partner was the majority owner and he would run the firm as he pleases. Great advice. I left and and subsequently founded a very successful and highly regarded consulting firm.
When the company that had acquired our niche software provider changed my network username from a name-based alpha to a nine-digit number.
Cruel management.
Realizing they owed me nothing, and I was simply in the way.
Missing a concert of one of my favorite performers to finish up something “critical” at work then driving home from the office so late that the sun was rising.
Promoted the worst director to be the new CIO.
Realization that in five years with an HIT consulting firm, we never once talked about “the patient.” Our mission statement was embarrassing to read.
Promoting and doctor to be the head of all IT clinical applications, over 100 people, when this doctor had NO experience being in charge of any size of team before, as he told all of us when he announced his promotion. No experience leading any organization whatsoever, no business or HR training, nothing. Talk about promoting someone to his level of incompetence. How often does leadership in healthcare think that just because someone is a doctor they can do anything?
A VP valuing contracts over business ethics and being completely detached from the realities of the marketplace, both in terms of realistic revenue targets and competitive compensation for our top talent, combined with a failing new product that was doomed from the start. The final acceptance of the fact that none of this was ever going to change was the “event.”
I left my last job because it was acquired by another company that was based in the South and I didn’t want to move from the SF Bay Area. Turns out to be the best decision.
A wholesale reduction of the middle management positions in the organization, making communication with manager more difficult (had too many direct reports to effectively manage); pushing many of our previous manager’s duties down on my team with no acknowledgement, support, or consideration of any type; and finally, removing almost any chance for future career advancement in this organization.
The CEO was corrupt (the controller quit rather than approve the yearly numbers), misused federal funds (set policy to have healthcare navigators sign up patients for ACA who were illegal using made up SSNs), racist (but because he was pro-Hispanic, it was not considered racism), did not support his leaders, required the implementation of the EHR when the environment was not stable and had not been thoroughly tested, and put blame on anyone who did not agree with him. The only reason I stayed as long as I did was due to the poor economy. It was a horrible situation to be in. The CIO was the only bright spot and he left soon after I did.
I am in sales and in a previous job sold well over $XXM and as deployment of the promised technology continued to fail, we were at a point with these clients of moving into Phase 2 of the project which would have netted the company another $XXM+ and the clients stopped everything. Lawsuits quickly began to fly. It was at this point I realized my leadership at this company was simply lying. They had done the Wolf of Wall Street. Created imaginary software that was incapable of supporting the demonstration they had put together with bubble bum and duct tape. I lost over half a million in commissions on Phase 2 because they had also conned me into believing they could make it work.
It is a train wreck in healthcare and amazingly complex. The demo experience worked flawlessly on their perfect data, but drop that bad boy vision into the reality of healthcare data and KABOOM. “Mr/s. Customer, you have to give us perfect data or this won’t work. Sorry, no refunds.” Plus, their contracts were unreal with one of the customers saying they were longer and more complex than the ones they worked through with their EMR vendor.
Unbelievable. Investors should have gone after that executive team with guns blazing in a lawsuit. They even made sales pump up pipeline numbers by telling us if anyone even picks up the phone, it is a 20 percent opportunity. Then post-acquisition, if you deleted those inflated opportunities, the same executive team (CEO) would literally email you within five minutes demanding an explanation.
When the going got tough, the C-suite exec refused to take responsibility for any of the struggles being dealt with by the staff that reported to him. In fact, he was quite adept at not listening and throwing people under the bus. Finally got to the point where I got on the bus and rode off to another job.
My company was purchased and I did not believe in the management or strategy of the acquiring company.
I found termination for cause suasive.
Toxic medical director, toxic culture , being treated like three year olds .
My director seemed to be semi-sabotaging our market install. At core team meetings, she would ask leaders whether they were on schedule, and upon hearing they weren’t, she would only say OK before moving to the next person. We were months and about a million over. She knew I thought we should ask people what the hold-up was, if they needed help, more training, etc. We had a planned core team meeting with the market CFO to give a status and tell him whether we felt on track and could make our live date. My manager came in to my office right before the meeting and told me to keep my mouth shut at the meeting. I sent my resume out the next week.
When my boss left, and HIS boss left within a day of each other. This was just after a new CEO took over.
My division was sold. The buyer offered a voluntary severance package within two weeks of the sale being final.
My company was acquired by a competitor. That’s probably the most obvious sign that’s it’s time to move on.
Our company was acquired. Marketing and accounting are the first to go.
Continually getting new “managers” who kept asking me how they should do their job.
When I realize the culture and the legacy leadership was never going to change.
My boss, the CIO of a large, multi-state IDN, falling asleep in my annual performance review.
New CEO hired through board member good-old-boy network was threatened by my skills and influence over the organization. Good thing my employment contract had a decent severance clause. CEO actually offered to extend the severance for signing a draconian non-compete agreement that went far beyond original employment contract. I turned him down. CEO was fired by the board a few months later after running the company into the ground with extravagant spending on a flawed strategy.
I decided to leave my job when I was told the CFO wouldn’t support me to be named the director of the business unit I was already leading. She would have to sign off on the position even though it didn’t report up through her. We had brought in $5m of unbudgeted money into the organization. It was a political mess and I am so glad that I left for a similar director position.
HHS appoints Genevieve Morris, MA as ONC’s principal deputy national coordinator. She was previously senior director of HIT policy with Audacious Inquiry.
Unlike her predecessor Vindell Washington, MD, Morris has no clinical education or experience (her master’s is in political science), having spent her nine-year career working on HIEs and Meaningful Use.
Reader Comments
From Significant Other: “Re: Partners HealthCare. I worked at Partners for many years and attended a February conference featuring CEO David Torchiana, MD (who had an insightful presentation, btw.) I asked the last question, which was ‘Can you talk a bit about Partners 2.0?’ His answer was quite candid — since its formation 23 years ago, little has been done to consolidate within the now $10+ billion organization. He expects to see a $500 million reduction over the next few years as the network reinvents itself. The Brigham and Women’s Hospital early retirement offering has nothing to do with Epic and that cost.”
From Hospital Personality: “Re: Epic. Announced that they are developing a fetal monitoring solution so that customers don’t need to turn to a third party such as Perigen, GE, or Obix.” Unverified.
From Diego: “Re: hospital MU3 attestation for Athenahealth users. For the Athenahealth spokesperson, how many of the company’s stated 35 live hospitals are using the complete inpatient solution, including clinicals? How many have actually attested with the inpatient product? How many users have fully implemented the inpatient product, including clinicals, within a 12-month timeline with the past two years?”
Epic’s App Orchard
I received more reader comments about working with Epic’s App Orchard.
#1
The experience with App Orchard thus far has been very disappointing. After paying the hefty fee for the Silver tier, we expected to receive all of the perks of the tier as discussed in the App Orchard documentation. Unfortunately, upon receiving access to the App Orchard program, it became readily apparent that much of what was promised was either not available or, in some cases, not yet built. Additionally, we were informed by App Orchard personnel that our "Sandbox" access would only be for a testing Sandbox and not an environment that we could use to demonstrate our solution to clients. The original documentation was highly misleading on this point.
The documentation also suggested that any press releases were to be submitted to the App Orchard team for review. After we went through a lot of effort constructing a press release with our PR firm and submitting it to App Orchard personnel for review, we were told that Epic would be providing developers with a standard press package.
All of this inconsistency is making us very uneasy. While we appreciate that we are one of the first few companies to join the App Orchard, and that we will be helping define the process for other companies in the future, we expected the process to be far more robust and established.
On the plus side, the App Orchard personnel have been very responsive and have provided as much help as they could given the under-developed state of the Orchard at the moment.
#2
We applied to the Epic App Orchard right when it was opened to vendors. Our initial interaction with Epic required us needing some detailed information on the different levels that App Orchard offered. I was pleasantly surprised to see how quickly they replied and how helpful they were as we worked through this decision.
Our application was processed timely and we got the access that we needed to start working on the technical integration. We are currently working on the technical integration and will soon be planning the marketing efforts. So far, so good.
#3
The team has been very responsive and the APIs are robust. We wish there were a bit more clarity on the pricing model for the live application (transactions vs. revenue share structures are a bit hard to follow). We also wish we had a clear sense of the timing / duration of the approval process for an application, as well as acceptance / rejection criteria.
HIStalk Announcements and Requests
Mrs. G’s DonorsChoose grant request was for STEM and engineering kits for her elementary school’s Robotic Rumblings program, noting that the city-wide STEM science fair includes few minorities and females. She reports, “The materials obtained through DonorsChoose are having quite an impact on my students. They are giving my students the opportunity to grow in the area of robotics. Their creative juices are definitely starting to soar. They are thinking and developing deeper thought processes on how to manipulate the materials. They are also learning how to better work together cooperatively. The students like working in small group settings. They appear to be quite focused when using the materials and do not want to leave when the session ends. We thank you from the bottom of our hearts. There are definitely some rumblings going on around here!!!!!!”
Webinars
None scheduled soon. Previous webinars are on our YouTube channel. Contact Lorre for information on webinar services.
Acquisitions, Funding, Business, and Stock
NantHealth reports Q1 results: revenue up 16 percent, adjusted EPS –$0.24 vs. –$0.18, missing expectations for both. NH shares continued their slide on the news, now down 83 percent since last year’s IPO.
Specialty EHR vendor Modernizing Medicine raises $231 million in a private equity investment, increasing its total to $322 million.
People
New York-Presbyterian promotes Peter M. Fleischut, MD to SVP/chief transformation officer.
Ivenix promotes Jesse Ambrosina to COO, George Gray to CTO/VP of R&D, Janice Clements-Skelton to VP of HR, Carolyn Malleck to VP of finance, and Ben Powers to VP of infusion systems.
Announcements and Implementations
PokitDok will build its healthcare transaction recording platform on the Linux Foundation’s open source Hyperledger Sawtooth blockchain project along with Intel Software Guard Extensions.
Vermont Information Technology Leaders and Medicity connect the Vermont HIE to the Veterans Health Information Exchange, allowing clinicians in the VA and the HIE members to view each other’s records for a veteran patient.
MModal announces enhancements to its computer-assisted physician documentation technology.
WellSpan Health brings its initial sites live on Epic.
Government and Politics
Officers in West Virginia’s state capitol arrest a veteran journalist who was attempting to ask HHS Secretary Tom Price if domestic violence would be considered a pre-existing condition under the House’s American Health Care Act. Dan Heyman was taken away in handcuffs and charged with “willful disruption of state government processes,” with the Secret Service agents who were protecting Price and White House Special Counsel Kellyanne Conway claiming they had warned Heyman that he was interfering with their work by shouting questions that Price was ignoring.
HIMSS reports that while Congress’s spending bill still won’t allow HHS to spend money to develop a national patient identifier, it encourages HHS and ONC to provide technical assistance to non-governmental organizations trying to address the patient identification issue.
President Trump threatens to withhold $7 billion per year in ACA cost-sharing reduction payments to insurance companies, which would likely drive more insurers out of the exchange market or raise premiums. The President said in an interview, “There is no Obamacare. It’s dead. Plus we’re subsidizing it and we don’t have to subsidize it. You know if I ever stop wanting to pay the subsidies, which I will, anytime I want.”
Privacy and Security
Memorial Hermann Health System (TX) pays $2.4 million to settle HIPAA charges following a 2015 incident in which it issued a press release that named an illegal immigrant who was arrested after using a phony Social Security card at one of its clinics. The hospital said it called police because of concerns about fraud, not immigration status. The woman’s husband was also in the country illegally, but had insurance through his employer.
Hackers breach two old data servers of a Memphis, TN family medicine practice using valid login credentials and demand a $10,000 ransom after encrypting its files, which the practice declined to pay since they switched EHRs 18 months ago and only those older records were involved.
Innovation and Research
Cerner says it’s interested in just-announced Microsoft technology that can identify, name, and index objects depicted in photos or video, saying it could be useful for alerting hospital nurses of patient actions that require their attention.
Other
Healthcare Growth Partners analyzes the valuation differences for enterprise vs. healthcare software as a service companies, concluding,
If the set of health IT companies were able to grow more quickly, it is likely that their valuations would become more in line with general enterprise SaaS companies. The reason for health IT’s slow growth rate is no doubt a complex combination of factors including longer sales cycles, heavy regulation, and slow adoption rates. Potentially it may be due to the relative immaturity of the healthcare software market and a different mix of publicly traded comps in health IT as compared to the larger and more mature enterprise SaaS market.
Sonar studies at University of Mississippi Medical Center (MS) reveal that up to 7,000 human bodies are buried on the hospital’s grounds, believed to be those of patients who died in the state’s mental hospital from 1855 to 1935 when it was located on what is now hospital property. Construction work turned up 2,000 bodies three years ago. The medical center, faced with a $21 million estimate to relocate the remains, is proposing to exhume a few of them for research and then just build a memorial.
A scientific editor trolls one of the many predatory medical journals with lofty-sounding titles that will run articles from publication-desperate researchers in return for cash. He submits an article built entirely around “Seinfeld” episodes as researched at the prestigious Arthur Vandelay Urological Research Institute, listing himself as the primary investigator under the name Dr. Martin van Nostrand. The Urology & Nephrology Open Access Journal accepted the article about a made-up condition nearly verbatim, billing him for its $799 fee (a mistake on their part since he declined to pay).
Eric Topol interviews the fascinating Pardis Sabeti, MD, PhD: member of a family who emigrated from Iran just before its 1978 revolution, Rhodes scholar, physician, scientist (computational biology and medical genetics), host of an education TV series about statistics, and singer/songwriter for Thousand Days, a decent alt-rock band.
Sponsor Updates
Advisory Board Chief Medical Officer Dennis Weaver, MD, MBA presented “Pragmatic Approaches to Succeed at Value-Based Payment and Care” at the World Health Care Congress Hospital and Health System Summit in Washington, DC last week.
EClinicalWorks will exhibit at the Ohio Association of Health Plans Annual Convention May 16-17 in Columbus.
GE Healthcare will supply over 200 Egyptian hospitals with 700 units of its advanced healthcare technologies.
Healthwise will exhibit at the Cerner Collaboration Forum May 16-18 in Kansas City, MO.
Huntzinger Management Group’s William Reed is named a Life Fellow Member of HIMSS.
Consulting Magazine names Impact Advisors VP Lydon Neumann one of the Top 25 Consultants of 2017.
Imprivata will exhibit at VA Healthcare 2017 2017 May 15-18 in Arlington, VA.
Entrepreneur Magazine features LogicWorks CEO Kenneth Ziegler.
Healthgrades recognizes Meditech hospitals for patient safety.
National Decision Support Company will exhibit at WEDI 2017 May 15-18 in Los Angeles.
Navicure and PatientKeeper will exhibit at Centricity Live 2017 May 17-20 in Boston.
Shane McCarran joins Orchestrate Healthcare as senior recruiter.
Experian Health will exhibit at HFMA WV May 17-19 in Roanoke.
InterSystems will exhibit at the NEHIMSS Annual Spring Conference May 11 in Foxboro, MA.
The US Patent Office awards Intelligent Medical Objects a patent for its medical terminology solution.
A DataBreaches.net investigation finds that up to several million records of Bronx-Lebanon Hospital Center (NY) were exposed after its revenue cycle contractor, iHealth Innovations, apparently misconfigured an rsync backup
Reader Comments
From Dr. Evil: “Re: EviCore. The specialty benefits manager is considering a sale or IPO, valuing itself at $4 billion. It pays to build a business around denying care.” The company describes its services as “comprehensive care management solutions,” although the emphasis seems to be on reducing cost via evidence-based solutions. It’s a good approach, although it fails to address out-of-control provider, drug, and device costs and instead focuses on restricting what is ordered. It’s an often-missed point that all of the political wrangling over health insurance would be much less necessary if costs were made reasonable, an even more daunting and therefore unlikely legislative accomplishment since the folks making fortunes on the backs of sick people also employ lobbyists.
Epic’s App Orchard
I received these unverified reader comments when I asked for first-person experience with Epic’s App Orchard.
I have worked extensively with Epic Corp over the past two years with their iterations of the App Orchard. The rules of the road require that an app developer permit Epic to take whatever IP they choose, if Epic believes it makes sense to include in future releases of Epic software. Epic will reject apps that directly compete with Epic functionality, as determined by Epic’s current and future roadmap. Further, the 30 percent fee they charge is too broad in scope for the app revenue (if there is any). Most importantly, originally, only Epic clients could submit apps to the Orchard, effectively locking out the global collective genius of non-Epic entrepreneurs (I am not sure if such a restriction remains). Based on the approach to their App Orchard, Epic seems to be trying to respond to the market demand for "open" as heavily advertised by Cerner as their competitive differentiator. However, Epic also seems to want to control the Epic app environment and has absolutely no motivation to loosen their model to the wild, as Judy mentioned several times that such a move would be the end of Epic.
We have started working with Epic to build out an API integration under the App Orchard. For us, the biggest concern are the revenue sharing terms. For a software vendor that is operating under tight margins in a competitive market, having to factor in up to a 25 percent gross revenue share is an impossible burden. From our perspective, the App Orchard is a blatant money grab from companies trying to innovate on the edges of the Epic ecosystem.
HIStalk Announcements and Requests
Welcome to new HIStalk Platinum Sponsor Softek Solutions. The Prairie Village, KS-based company’s OnTrack software and consulting services optimize revenue integrity and system performance for Cerner Millennium hospitals (and those preparing to move to Millennium). Its Charge Integrity Control provides visibility into revenue management by correlating patient orders and charges throughout the transaction process –one customer found a lab charge error that lost them $3 million in appropriate billing over four months before they found it instantly with Charge Integrity Control. Revenue Conversion Services allows correction of application, workflow, and configuration problems that otherwise would cause millions of dollars in lost revenue right after a Cerner go-live — a single hospital called Softek three months after go-live and avoided $20 million in annualized lost charges due to orders that weren’t charging, a location-specific workflow problem with ordering, and ED batch charges that weren’t actually charging. The company also provides Millennium system performance optimization software and services as well as conversion and purge maintenance assistance using proprietary diagnostics. Thanks to Softek Solutions for supporting HIStalk.
I finally pulled the trigger on replacing of my years-old, $300 laptop that I use for everything. I chose an Acer Aspire E15, which has pretty decent specs for $621: an AMD FX 9800p CPU with 2 MB L2 cache, 16 GB of DDR 4 SDRAM, a 128 GB solid state drive running Windows 10, a 1-terabyte hard drive for data, a 15.6-inch display powered by a Radeon R8 dual graphics video card with 2 GB of dedicated VRAM, and thankfully nearly zero pre-installed bloatware. I’ve had no problems so far getting it loaded up.
HIStalk readers funded the DonorsChoose grant request of Mrs. S in California, who asked for a 3Doodler child-safe 3-D printing system (it was actually inexpensive at just $113 for everything, plus our donation was matched). She reports, “I would like to thank you from 22 very excited third grade students that have really been enjoying and benefiting from your generous donation! We have been using our 3Doodler pen each Friday afternoon during our STEAM centers time and I have truly observed some fantastic skill building. Some of the benefits that are very noticeable to me are an increased attention to detail, improved direction following within a detailed task, increased patience for a task, increased observation of the steps necessary for a positive outcome, and an increased motivation to try something new! You have made a difference!”
Webinars
None scheduled soon. Previous webinars are on our YouTube channel. Contact Lorre for information on webinar services.
Acquisitions, Funding, Business, and Stock
Video visit provider Teladoc reports Q1 results: revenue up 60 percent, EPS –$0.30 vs. –$0.40, beating analyst expectations for both.
People
Reed Liggin (Athenahealth) joins electronic prescribing system vendor EazyScripts as CEO. He was president and CEO of the small-hospital information system vendor RazorInsights that was acquired by Athenahealth in January 2015.
Telehealth solution provider Avizia hires Joe Quinn (ComScore) as CFO.
Health Symmetric hires Bob Teague, MD (Quorum Health Resources) as chief medical officer. The company’s website uses a lot of vague gibberish in not saying exactly what it is they’re selling other than a “healthcare platform” that uses APIs.
Announcements and Implementations
Intelligent Medical Objects is awarded a patent for its concept-based terminology management system that allows rapid distribution of terminology changes to the company’s EHR vendor partners. Clinician-entered terms are matched with appropriate billing and reference codes that capture clinical intent.
Hybrid IT vendor TierPoint will expand its Hawthorne, NY data center campus for the third time, adding 38,000 square feet of raised floor to the existing facility that includes 52,000 square feet of raised floor plus a 70,000 square foot recovery and business continuity center.
PeriGen releases PeriWatch, a perinatal analytics system that integrates WatchChild fetal monitoring with PeriCALM decision support and adds a maternal dashboard.
Penn Medicine Center for Health Care Innovation (PA wins ECRI Institute’s health device award for its app development platform that extracts clinical information from the EHR and other sources.
Government and Politics
In England, the Cambridge University Hospitals trust will decide this summer whether to outsource commodity IT services that include enterprise infrastructure, service desk, and end-user computing in a tender expected to total $180 million over seven years. The trust says its increasing Epic use has created a need to expand its services.
The White House appoints Gopal Khanna (Illinois Department of Innovation and Technology) as director of AHRQ.
Innovation and Research
University of Illinois at Urbana-Champaign is working on a virtual physician agent that can describe lab test results to patients via a patient portal, targeting older adults with conversational speaking, context-appropriate facial features, and other body cues that can help with retention.
Other
St. Mary’s Hospital (NJ) celebrates Nursing Week by laying off seven nurses and 13 med techs.
Sponsor Updates
The local paper profiles Ability Network CEO Mark Pulido.
Black Book identifies 10 top MACRA trends challenging providers with value-based care and quality metrics.
Agfa Healthcare launches a new version of its Integrated Care Suite.
Besler Consulting releases a new podcast, “Healthcare in the first 100 days of the Trump presidency.”
Washingtonian names The Advisory Board Company CEO Robert Musslewhite as one of its biennial Tech Titans.
Casenet announces its Connect 2017 speaker lineup, led by client executives from Cigna and Healthfirst.
CoverMyMeds will exhibit at the American Academy of Ambulatory Care Nursing Annual Conference May 10-13 in New Orleans.
Boston Software posts a white paper titled “Eliminate the Pain of EMR Upgrade Testing” that describes use of its Cognauto system to validate and set appropriate expectations for each department regarding the added benefits of the EMR upgrade.
The Hartford Business Journal interviews Diameter Health CEO Eric Rosow.
Health Professional Radio interviews Docent Health co-founder Paul Roscoe.
Stakeholders react to news that HHS will launch a healthcare cybersecurity center this summer. By @JennHIStalk
While administrations may change and legislation come and go, the need for cybersecurity across healthcare’s many verticals seems to be a constant that will remain with the industry for the foreseeable future. News that HHS will create a Healthcare Cybersecurity Communications and Integration Center this summer highlights the federal government’s commitment to helping providers, payers, vendors, and (hopefully) patients prevent data breaches that could impact patient safety.
Modeled after the Department of Homeland Security’s National Cybersecurity and Communications Integration Center, the new HHS center helps to fulfill the Cybersecurity Information Sharing Act of 2015, part of a broad initiative under the Obama administration to bolster the government’s offensive and defensive cybersecurity capabilities.
“HCCIC establishes the mechanism to provide proactive and anticipatory analysis of cyber threats to both HHS and the healthcare and public health sector,” says an HHS spokesperson. (The department declined a formal interview.) “The HCCIC will act as a clearinghouse to drive healthcare-relevant cyber indicators, briefings, and actionable intelligence to and from a wide variety of stakeholders – both public and private. HHS aims to begin initial operations this summer.”
The timing is apropos given the impending release of a report authored by the Health Care Industry Cybersecurity Task Force, a CISA-mandated group put together last spring tasked with:
Analyzing how other industries have addressed cybersecurity threats.
Reviewing the security challenges associated with networked medical devices and software connected to EHRs.
Developing and circulating cybersecurity best practices.
Establishing a plan the government can use to freely share real-time intel regarding healthcare cybersecurity threats.
While HHS would not confirm the HCCIC will help to implement the task force’s recommendations, one can only assume that the two resources will converge to some degree. Industry stakeholders are of course eager to collaborate and benefit from the new center’s deliverables, which are yet to be fully determined.
“We are anxious to begin to see actionable data coming out of the HCCIC, including threat and vulnerability,” says Marc Probst, CIO of Intermountain Healthcare (UT), which formed a cybersecurity center last year with the University of Utah and several other partners. “The HHS goals around information sharing and analysis align perfectly with our organization and several that we are working with,” he adds. “We are anxious to contribute and develop automated feeds for the HCCIC.”
While emphasizing that long-overdue federal cybersecurity risk assessment and risk management efforts will provide good implementation guidance, Probst and his colleagues are reluctant to see cybersecurity become a compliance effort or a certification program. “Many of those currently participating are vendors or people with a product to sell,” Probst explains. “We hope the committees and chairs will seek more payer and provider participants.”
While selling a product to providers in need would surely be seen as a positive outcome for any vendor involved, Divurgent CISO Stephen Watkins sees the benefit of an HHS-sponsored cybersecurity center as one of cohesive collaboration. “For advisory and consulting services organizations like ours,” he says, “these centers allow us to share and contribute our strategic, operational, and tactical insight from the field as well as act as both sounding boards and feedback loops for best-practice implementation guidance from the HCCIC, especially for small providers that may not have in-house IT security staff.”
Real-time cybersecurity guidance to the healthcare community will surely be welcome in light of today’s constant stream of data breach announcements, which have become so banal as to no longer incite the media hysteria it first engendered a year or two ago. While it may be too much to hope the center and its collaborators can help providers, payers, and vendors stay ahead of constantly evolving cyber threats, stakeholders no doubt hope HCCIC resources will become some of the strongest defenses in their cybersecurity arsenal.
Billionaire investor Warren Buffett says in the annual Berkshire Hathaway shareholders’ meeting that the American Health Care Act would be “a huge tax cut for guys like me,” adding that, “Medical costs are the tapeworm of American economic competitiveness.”
Buffett also complained that private equity firms load their acquired companies with debt, announced that the company has sold one-third of the IBM shares it holds, and joked in answering a question about how much his successor will be paid (Buffett is 86) that, “If the board hires a compensation consultant, I’m coming back.”
Reader Comments
From Chiming In on CHIME: “Re: CHIME. You asked why people are quitting HIMSS. I’d like to see the same anonymous question about why people are quitting CHIME. I’m considering it since it has changed from a CIO networking organization to a vendor-driven one, where companies pay for CIO time.” I created a rather awkwardly worded survey here and will report the results next week.
From 300-Buck Gyp: “Re: radiology report. A friend’s pelvic CT scan had this radiologist comment in the report: ‘CT pelvis. Reproductive organs – the uterus and ovaries are normal. I guess the fee includes copy/paste issues since the patient is a male.” Perhaps “normal” could be loosely construed as meaning that the lady parts are “absent” in male patients, thus streamlining the radiologist’s report template even more.
From Privy Pathway: “Re: Brigham and Women’s. Any thoughts on the offering voluntary buyouts as a cost-cutting measure? It used to be that Epic only got the C-suite fired, but Brigham, MD Anderson, and Southcoast are proving a trend. I’ve also heard that a notable health system is cutting annual compensation increases for the rank and file given capital and operating constraints associated with their Epic go-live.” My cheap-seats view would be this. Epic is fanatical about forcing customers to budget the entire project’s expense. My survey of C-level execs of health systems that use Epic (which got pretty big participation) found that 75 percent of projects came in at or under budget, with just 15 percent saying they spent a lot more than they expected. Therefore, I’ll postulate that it’s probably simplistic to assume that Epic is guilty just because it was present at the crime scene:
Health systems that choose Epic should not be surprised by its upfront and ongoing costs. That would seem to be the case with most of its customers since few have had disastrous, permanent financial challenges purely because of Epic, especially those that have been live for a few years.
Leaders of financially challenged hospitals typically find a scapegoat, whether it’s unions, government payments, IT, or regulatory compliance costs. They haven’t blamed Epic all that often, but even when they did, the reality might not be quite so simple, especially if the executives are looking to justify unpopular decisions.
The type of health systems that choose Epic (large, aggressive, market-leading health systems) are those most likely to have had their bottom line hit by government, payment, and marketing challenges as the emphasis shifts away from heads in the bed and the extraordinarily high cost of hospital-provided care, especially in those with massive market clout that drives negotiation with insurers.
Timing is everything. Epic gained a lot of customers in the past 3-4 years and financial conditions have changed considerably since then, so those significant upfront costs may be hitting at an inopportune time for some health systems.
Having poor financial performance after Epic doesn’t necessarily mean Epic was the problem. Some hospitals screwed up their implementations with bad decisions, while others were poorly managed both before and after Epic. Sometimes you read about a high-profit health system choking on Epic and think to yourself, based on what I know about them, I’m not too surprised they managed to mess it up. Software ROI is usually more related to the client than the vendor.
Some of the hospitals are cutting back because of future expectations, not necessarily due to concerns about their current bottom lines.
It’s going to get a lot worse of the ACA is repealed and many millions of hospital patients go back to being charitable write-offs, shrinking health system profits.
HIStalk Announcements and Requests
Nearly 80 percent of poll respondents haven’t bypassed insurance to pay cash for a better ongoing PCP. Stephen pays an $149 annual fee to belong to One Medical even though the actual visits are still covered by insurance. Nonsequitur took the concierge route for his father since few decent doctors in his area accept Medicare, adding that the new practice provides nearly 24/7 secure communications via Twistle. Amy says she hasn’t done it for a PCP, but does so for other services because some providers offer a cash price that’s cheaper than paying her high-dollar insurance deductible. Rose goes out of network to keep a particular PCP even as insurance contracts change frequently, although she’s cautious to get orders for expensive lab and rad tests ordered by an in-network provider since some plans won’t pay for them otherwise.
New poll to your right or here: what was your reaction to the House’s passage of the American Health Care Act last week? Feel free to elaborate further by clicking the poll’s “Comments” link after voting.
HIStalk readers provided an Amazon Fire TV and accessories for Ms. D’s California elementary school class in funding her DonorsChoose grant request. She reports, “Technology is always changing, so my teaching strategies need to accommodate the needs of my students. Most of them are visual learners, so I play YouTube clips and videos all the time when I am teaching science. In addition, the Amazon Fire TV has allowed my students to visually see the concept as they are watching science videos on TV. Now, my students are extremely excited about science! On behalf of my students, thank you for supporting them as they continue to reach for their goals!”
This Week in Health IT History
One year ago:
Theranos announces a reorganization that includes the retirement of President and COO Sunny Balwani.
HHS spells out details of its proposed MACRA program.
NextGen ceases development of its NextGen Now cloud-based PM/EHR as it moves focus to its acquired HealthFusion product.
The FDA rejects the application of the “digital pill” that uses technology from Proteus Digital Health.
Apple releases the CareKit developer’s framework.
Internal documents from University of Texas indicate that MD Anderson Cancer Center blames its Epic implementation for a nearly 60 percent year-over-year income decrease, although noting that it had already assumed some negative impact.
Siemens changes the name of Siemens Healthcare to Siemens Healthineers.
Five years ago:
Partners HealthCare chooses Epic to replace Siemens Soarian.
ONC launches its Health IT Dashboard.
The Nashville Medical Trade Center names six companies that will join HIMSS as tenants.
Medseek announces plans to conduct a management buyout of the company.
Weekly Anonymous Reader Question
I asked readers to describe the best career advice they have received:
You can do better without working more hours.
From Ben Franklin: ask people for help in order to make them like you.
From my first professional manager who that had been employed for our then-current employer for the previous 30 years, "Don’t make the same mistake as me and think that you need to stay with the same company your whole career." Knowing what I know now, and having held various positions with several different employers over the course of 25 years, I would have loved the opportunity to have been given the option to stay put.
Perception is reality. It doesn’t matter what you think — if people perceive X, then X is true.
Always put yourself in the other person’s shoes — most people have good intentions, so if they don’t behave in a good way, understand why from their point of view.
When I was thinking of starting my own independent, HIT consultancy in 1985 — terrified every step of the way, but more terrified not to do it — my mentor at the HIT company where I was employed advised me that, so far, my track record for getting through rough days is 100 percent and that’s pretty good.
Be nice to the administrative assistants.
When you walk somewhere, go fast so you look like you’re actually on your way to do something.
Realize when it’s time to recalibrate. Your vision of your life when you were 18 is probably different than it has turned out to be when you reach 40, so focus on the accomplishments rather than regrets.
Being told that I was not a good writer, and as such would never be published in one of the B2B magazines owned by the publishing company I worked for. While not your typical piece of advice, I took it as a challenge to prove the naysayers wrong. I believe my ensuing track record of published pieces for a variety of media outlets speaks for itself.
My daughter just became an RN and has started working at our local hospital. In her first week or so, she was introduced in passing to an OB/GYN who happens to be my wife’s and also happened to be the doctor who delivered my daughter. She says "Hello, Dr. A," to which he replies "Get out of healthcare, kid."
People will always remember how you’ve made them feel. Don’t be a jerk.
Don’t listen to your parents. They really think they know you, but they can’t because you only become you by following your nose and that takes time, experimentation, trial and error, and the occasionally do-over. In fact, don’t listen to anyone. Do something that is new every day, and when it stops being new at least a little every week, then move on.
Listen. You may be the smartest person in the room. Listen anyway. You’ll learn something.
If it’s not going to matter in five years, it doesn’t matter now. Pull back and reconsider your response to the situation.
You need to read HIStalk.
When the horse has died, dismount. (Ross Perot)
Your boss cares about results, not the path you took to get there.
If you are young and take a travel job for the higher pay, have an exit plan. Otherwise, you’ll find yourself still on a plane traveling every week when you are 65 years old, having missed so many family and friends moments because you were always on the road.
You can love your job, but it will never love you back. No job — no matter how rewarding either financially or emotionally — is worth destroying your peace or sanity for.
Do not let one person ruin your job. (Advice I should have taken.) I left a job after 6.5 years because I could not stand my boss. Other people just ignored or tolerated him. Many of them are still there today, 15 years later. He has since retired.
Back in the early 1980s: learn to type. Sounds dated now, but as my mother said, you can always fall back on being a secretary if needed. Thankfully I took four years of typing in high school, and went onto college to get my bachelors. I type for a living now in IT.
Earlier in my career, I was really ambitious and wanted a promotion after my direct manager left. I wasn’t ready to be the department manager but i met with the VP making the decision anyway. He learned more about my background and experience and said to me, "You have to ask for the job you want, otherwise no one will know you want it." It was a revelation to me. A plain spoken truth and something so simple would be the best career advice I ever received.
My first CIO taught me not to ever say “no” to my business partners. Say “how long” what they want will take to acquire and/or develop, and “how much” it might cost. This is our obligation as IT professionals serving an organization.
Taking the path of integrity and good character will not always result in promotion within an organization. You must be willing to stick to your professional values and be ready to move on to new adventures if your superiors do not like your answers.
You hold yourself back more than anyone or anything. You are good at what you do. Have faith in yourself, be heard, make a difference.
Spend more personal time with your team. Show your human side. Both will build more trust, which will make the team closer and stronger.
Never talk to a reporter. Your response should always be "no comment."
Don’t do anything rash.
When you have an issue with the way the organization is being run, address it by tying it to core values or customers, not by calling out the way a specific person does things.
You should spend 10 percent of your time looking for your next gig.
Do what you say you’re going to do, when you say you’re going to do it. Return the call or email promptly even if you don’t have the answer. In other words, be there. If colleagues and customers know they can count on you, you’ll be given more opportunities (and responsibilities) to grow your career and, at the same time, build a network that will be increasingly valuable.
Arrive at a meeting at least five minutes early, and if you are leading, a meeting ensure that it ends on time or earlier.
I was having trouble getting what I needed professionally from a boss. The advice I received from a mentor was, "She will never be the kind of boss you need. So how do you make the most of what she has to offer and get your other needs met elsewhere?"
Live on what you currently make so your employer will never "own" you. I stayed in positions because I wanted to be there, not to get a paycheck.
Worry about the sale. The margin will take care of itself.
Advice to a just promoted CIO: "Remember that you are a VP of the organization, not just of IT."
Don’t apologize if you have not done anything wrong. Said to me by the late great Steve Macaleer, of the Macaleer/SMS family, who died way too young at 49.
Every five years or so, change jobs. You have probably developed bad habits that are best discarded. You can do this within your current employer or by getting a new employer.
Ninety-five percent of the time you are right, but 95 percent of the time your delivery sucks. You need to work on your delivery AND timing.
This week’s question: what specific event crystallized your decision to leave your last job? (or another previous job if you’ve got a good story from there).
Welcome to new HIStalk Platinum Sponsor CSI Healthcare IT. The Jacksonville, FL-based company, which has offered services nationally for 20 years, provides training and implementation solutions for EHR and coding as well as IT staff augmentation, legacy system support, and infrastructure staffing. Case studies: Houston Methodist (CPOE activation), Norton Healthcare (a 300-contractor Epic go-live), Sutter Health (Epic training), and Grady (big-bang Epic go-lives). The company’s consultants voted it to Inavero’s Best of Staffing Talent List, which recognizes fewer than 1 percent of staffing agencies in North America. The company provides customized consulting and staffing solutions that provide unmatched results at a fraction of the cost. Thanks to CSI Healthcare IT for supporting HIStalk.
Thanks to the following companies that recently supported HIStalk. Click a logo for more information.
Last Week’s Most Interesting News
The House passes the American Health Care Act that would repeal most of the Affordable Care Act, sending the bill to the Senate.
Thoma Bravo buys Lexmark’s Perceptive Software business and moves it under its Hyland Software portfolio company.
Computer systems at University Hospitals (OH) go down for several days due to unspecified causes.
ONC launches a patient matching algorithm challenge.
Meditech announces Q1 earnings per share of $0.39 vs. $0.51 in the same quarter last year.
Internal medicine physicians at Canada’s Nanaimo General Hospital are disciplined for going back to paper orders in declaring patient safety concerns with Island Health’s Cerner system.
Webinars
None scheduled soon. Previous webinars are on our YouTube channel. Contact Lorre for information on webinar services.
Acquisitions, Funding, Business, and Stock
From the Allscripts earnings call, following the quarterly report in which the company beat expectations on earnings and met on revenue:
A strong segment was Payer and Life Science.
The company expects its acceptance into the UK’s NHS London Procurement Partnership to help it maintain UK momentum.
The Netsmart acquisition contributed around $50 million of the quarter’s bookings.
Paul Black says the company is watching the market evaluation being performed by the VA and Coast Guard, noting that the Allscripts loss in the DoD bid wasn’t due to technology, applications, workflow, security, or company background – it didn’t make it to the final round because of price.
The company is not seeing the decline in claims volume as reported by Athenahealth, although it notes that Athenahealth has greater exposure than Allscripts because of its business model.
Allscripts will focus on increasing the client base’s adoption of Sunrise Financial Manager rather than trying to roll out outsourced inpatient revenue cycle management services.
Decisions
Central Montana Medical Center (MT) will switch from Evident to Infor supply chain management in 2017.
Children’s Hospital Of New Orleans will go live with Epic in 2018.
New Orleans East Hospital (LA) will switch from Cerner/Siemens Soarian to Epic in 2018.
Thomas Memorial Hospital (OH) replaced Siemens with Meditech on March 1, 2017.
These provider-reported updates are provided by Definitive Healthcare, which offers a free trial of its powerful intelligence on hospitals, physicians, and healthcare providers.
People
New York-Presbyterian Hospital (NY) promotes Rosemary Ventura, MA, RN, DNP to the newly created position of CNIO.
Announcements and Implementations
Reaction Data publishes its “Big Mega HIT Purchasing Report,” which finds that the top spending item of health systems and standalone hospitals in the next 12 months will be inpatient and ambulatory EHRs (Epic was #1 in mindshare for both, followed Cerner and Meditech that were nearly equal in score). Hospital-owned physician groups will focus on information security, while independent practices place telehealth as #1 with equal interest in four vendors.
Definitive Healthcare adds quarterly inpatient and outpatient Medicare claims data for hospitals, clinics, and long-term care providers to its provider data, intelligence, and analytics product line.
Government and Politics
VA Secretary David Shulkin reiterates that he will announce the VA’s plans for VistA in July, choosing to either replace it with a commercial system or turn VistA over to a private company to convert it into a single, cloud-based, externally managed instance. When asked about the historic lack of technology cooperation between the VA and the Department of Defense, Shulkin promised better, saying, “We’ve always found ways not to do that.”
Privacy and Security
Hacker The Dark Overlord posts records of 180,000 patients online from medical practice hacks last year, most likely because those facilities declined to pay the extortion demanded.
Other
A Utah-based orthopedic surgeon is ordered to turn over 10 website domains to Intermountain Health Care, which complained that the doctor had no legitimate reason to have purchased domains related to Intermountain’s Cedar City Hospital and was instead was trying to use them to convince an insurance company to add him as an in-network provider.
Here’s the finale of Vince and Elise’s series on physician practice vendors, this time looking at the “other” ones.








![image5[1]](http://histalk2.com/wp-content/uploads/2017/05/image51.png "image5[1]")







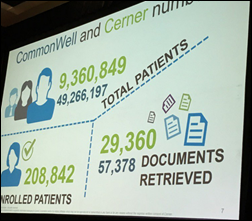







































































































































































































The news about AHRQ is very unfortunate. The AHRQ staff were always excellent to collaborate with. They had an impressive…