

News 3/11/09
From Paul Pott: "Re: grocery code barcode article. Didn’t you write some commentary awhile back? Maybe Dennis Quaid should read it …oh, wait, he is too busy solving the problem with his easy solutions." A couple of readers recalled a piece I wrote two years ago called Want to Anger a Nurse? Make Smug Coments about Grocery Store Barcoding. And regarding Dennis Quaid, I should say that I have no problem with his being mad, disillusioned, distrustful, litigious, and now vocal. Its HIMSS that I have a problem with, putting him onstage in an HIT keynote as though we are ignorant to medical errors without having a layperson challenging us at a conference, particularly one who suffered no loss other than some panicky moments (unfortunately, there are plenty of people whose experience with medical errors is far more tragic). Well, HIMSS has made some odd keynote choices before (Dana Carvey, for example) and I suppose this one’s no worse when the objective is simply to pay a big celebrity to bump up the cool factor. Maybe he’ll do something interesting like have someone from Cedars on stage with him (I’m predicting that).

From xtremegeek: "Re: Akron General Hospital. Heard they laid off over 100. Can anyone confirm?" The body count was 145, according to an article in today’s Plain Dealer.
Fountain Valley Regional Hospital (CA) is using video-equipped robots to connect doctors with patients. It is law that every IT system intended for nurse use must have a contrived acronym name chosen by contest (as a thinly disguised ploy to increase rank-and-file support, of course, and highly insulting to nurses if you ask me), so theirs is called ERNI. A patient is quoted: "They said a doctor was going to talk to me and then it came wheeling around. I just figured that was the new era. I didn’t feel like it was impersonal at all."
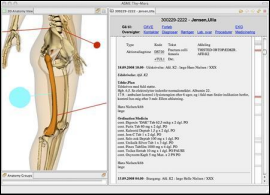
IBM works with a hospital in Denmark to develop a 3D anatomical view of available EMR information, allowing doctors to click on a body part to drill down into related information. Sounds cool, although I don’t see how it affects outcomes.
Analytics vendor Enclarity raises $5.5 million in Series C funding, bringing its total to $22 million.
Marlin Equity Partners acquires billing and collections vendor MDeverywhere, adding it to a stable that includes MedAvant. I Googled HIStalk to see if I’d mentioned MDeverywhere previously and darned if I didn’t mention a company by that name (maybe not the same one) in my 12th-ever HIStalk post, June 30, 2003. That was right after I boldly predicted that Epic would no longer be a serious HIS competitor because it had just signed the Kaiser deal (which I also predicted would fail). Well, I was young and foolish and so was Epic back then, so you will have to forgive us both.

Thanks to GetWellNetwork of Bethesda, MD, a brand new Platinum Sponsor of HIStalk. Premise Chairman CEO Eric Rosow (now Eclipsys) introduced me by e-mail to GetWellNetwork Founder and CEO Michael O’ Neil, we did a Moment With, and he must have gotten a lot of response because here they are a new sponsor. The company sells interactive patient care solutions (bedside education, safety, pathways, pain assessment, etc.) and patient entertainment and communication systems. I appreciate their support.
The medical director of O’Connor Family Health Center (CA) tries to make the best of its transition to an EMR, saying he doesn’t regret it despite (a) the fact that it cost $250,000 and required an army of people; (b) patient backlog was up and revenue down for three months after go-live; and (c) their vendor has gone belly-up since their implementation and product support ends in two years. I bet that particular Mrs. Lincoln really liked the play.
I bet HIMSS was hoping for some rosy survey results about ARRA after all the cheerleading it did for it, but HIT professionals think differently: only a third of them believe all those HIT stimulus provisions will end up saving healthcare dollars.
Thanks to those who RSVPed for our HIMSS reception and apologies to those who missed the cutoff (some folks took heed when I wrote Saturday that the cap was imminent). The most common titles of attendees: VP/EVP/SVP/RVP (76), CEO/Chairman (45), and Director (40). I’m happy to see that some of my provider-sider peers jumped in there too, with some doctors, nurses, IT people, and CIOs. Title counting aside, thanks to every single person who signed up – it means a lot to me. It never ceases to amaze me that people pay at least a little attention to an anonymous blogger who’s sticking to his nonprofit hospital IT day job (as some of you less impressed readers have recommended).
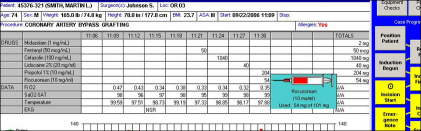
A reader had posted a comment about IntrinsiQ, the folks who sell the IntelliDose oncology system. Inga connected with Jeff Forringer, the company’s new president, who was good enough to provide a response. "Thanks again for reaching out to me directly. As I said in my initial response there is no planned reduction in force for 2009. As a matter of fact we plan to invest even more in software development and client service this year. Overall I think you’ll be happy to hear where IntrinsiQ is heading – especially given your concerns about the ongoing importance of our clinical software business. While we’re still putting the operational roadmap in place to achieve our goals, here’s an overview of our vision. (a) Extend the improvements we made in version 3.8 to the e-nurse and charge capture modules to the order writing module in our 3.9 version this year. (b) Use these changes in the underlying architecture to develop a light version of the product that can be used by smaller facilities. (c) Continue our cooperative approach with full service EMR vendors to be the oncology module that makes their systems better. (d) Use our data processing and analytical skills to provide sites with information about how they practice and how that compares to the rest of the country. (e) Develop new modules and services that help sites improve the quality of care. On the software management side I have made two changes. I hired Rich Gray as the GM of our software division. Rich was with IntrinsiQ for a number of years and has rejoined. Rich’s experience with the software, healthcare IT space and his clinical background are a great addition to the team and will help us reach our goal of becoming a bigger part of helping sites improve the quality and understanding of care The other management change that I made was to promote Steve Hamann to the management team. Over the past 2 years Steve has led the effort to improve IntelliDose’s user interface and the underlying architecture. I hope this gives you and ideas of where we are headed. I would be happy to talk more about what we would like to do long term, the commitment of our board to the process and how the software and data business work together if you are interested."
Philips expands its headcount by 30 in its Belfast office, the Northern Ireland location that was formerly part of the acquired Tomcat Clinical Systems.
QuadraMed announces Q4 results after Tuesday’s market close: revenue down 6%, EPS $0.14 vs. $0.52 (after excluding a one-time tax treatment from last year).
We did an interview with Cheryl Iseberg, COO of Renaissance Resource Associates, an HIStalk Platinum Sponsor that provides consulting services for GE Centricity Enterprise, Picis, Epic, and other systems.
Another example that consumers don’t think doctor bills are real: someone complains to a TV station that if a doctor doesn’t write off charges for a test his insurance company said he didn’t need (after refusing to pay for it, of course), his credit score will suffer because he’s not planning to pay the bill.
Jobs: Project Office Manager (NC), MEDITECH Financial/Billing Expert (national), Director of Business Systems (CA), MEDITECH Consultant – Advanced Clinicals (national).
A RAND Corporation study says pay-for-performance plans sell a lot of IT, but haven’t improved healthcare quality, based on its review of a big California project. The problem: doctors weren’t interested in major change when only a couple of thousand dollars a year was at stake.
MEDSEEK is offering a free Webinar in its series on eHealth, this one on Wednesday, March 18.
Southern Arizona HIE is working with Wellogic to roll out more electronic patient information. Also mentioned: it hopes (like everybody else) to get a slice of the Obama Pork Pie (actually, I shouldn’t say that since I’m almost but not quite convinced he had no choice).
CVS Caremark closes 16% of its MinuteClinic locations, placing them on a "seasonal schedule" to supposedly reopen later. I’ll give its PR people credit for putting a positive spin on closing stores because of poor sales: they are doing it "to align with consumer demand."
The Conficker worm is still out there, infecting networks at two hospitals in Scotland last week and requiring a two-day downtime that forced the rescheduling of cancer patients.
Maybe this is an argument for EMRs: the family of a 60-year-old woman who died of an E. coli infection gets a $2.6 million jury verdict from a hospital. They had taken the patient to the ED, which drew positive blood cultures, but the nurse put the paper result in a folder on the doctor’s desk, where it went unreviewed for 12 hours.
HERtalk by Inga
From Spicey: “Re: HIStalk/Ingenix reception. You guys should be flattered it’s sold out … everyone thinks this is the ‘must do’ of HIMSS!” We are flattered that so many want to attend this sure-to-be-fun event hosted by the wonderful Ingenix folks. I hear the location (Trump Hotel) is gorgeous and I am sure the food will be divine. If, by chance, you did RSVP and your plans change, let us know if you can’t make it. We’d love to free up some spots for people who missed the cutoff (some of whom are e-mailing frantically hoping to get squeezed in, but we have a space limit).
From Shoe Diva: “Re: HIMSS footwear. I went shopping a couple of weeks ago for comfy shoes … none of those beautiful shoes for me. I swore last year I would resort to black tennis shoes. What about you?” This is one of life’s biggest dilemma: function versus fashion. Why can’t someone design a gorgeous shoe that you can walk around in all day without killing your feet and your back? And, that is also suitable for Chicago’s potentially frigid weather?
Speaking of HIMSS, the obvious buzz this year will be around HITECH, including how each vendors have the perfect solution and what providers will need to do in order to get their money. Coming in a distant second, I predict a good deal of talk of products and services to help providers adapt to a more consumer-driven healthcare world. Next, look for cool ways to use your PDA.
Thirteen hospitals reach HIMSS Stage 7 EHR ranking and all but one are part of Kaiser Permanente. NorthShore University HealthSystems (IL) was the other system to make the list for three of its four campuses. Interestingly, all Stage 7 honorees use Epic for their core HIT system.
A new study suggests that as many of half of the country’s physicians will determine that HITECH financial incentives are not enough for them to move forward on EHR adoption. Avalere estimates that the average solo or small group practice will spend $124,000 over five years to adopt EHR and will receive $44,000 in incentive payments. That’s a $14,000-a-year deficit compared to an estimated $8,500 a year Medicare reimbursement penalty for non-adoption. The biggest problem with this argument, however, is that it does not address any potential savings and efficiencies physicians gain as a result of implementing EMR, such as reduced transcription costs, savings on charts and chart storage, lower malpractice rates, etc. And what about the value of improved patient safety?
Health Systems Solutions announces it will de-register its common stock and stop filings with the SEC following the collapse of its planned Emageon merger and the fraud investigation of its principal investor.
The US unemployment rate continues to climb and now sits at 8.1%. Meanwhile, healthcare remains one of the few bright spots, adding 27,000 more jobs in February.
Integration firm Bostech Corporation partners with HIT consulting firm Orchestrate Healthcare to promote open and integrated healthcare technology solutions.
Allscripts-Misys finds a buyer willing to pay $26 million for its medication services business. A-S Medication Solutions will pay Allscripts $8 million in the 4th quarter and $3.6 million per year over the next five years in return for A-S sales and marketing services.

St. Joseph’s Hospital Health Center deploys RelayHealth’s IntegrateRX Prescription History to aid with medication reconciliation.
CHRISTUS Health implements Picis LYNX E/Point in 18 of its acute care hospitals and plans to add three more sites soon.
The Department of Justice files suit against Community Health Systems (CHS) for allegedly defrauding Medicaid of $47.5 million. A whistleblower originally alerted officials of possible fraud after three New Mexico hospitals and CHS allegedly collected disproportionate share payments to which they were not entitled.
The 235-bed Children’s Hospital (LA) successfully installs Sunquest LIS specimen Collection Management and Encompass Web-based ordering, resulting, and reporting systems.
Satyam Computer Services starts a competitive bidding process to find an investor willing to acquire a majority stake in the scandal-ridden company.
Memorial Hospital and Health Care Center (Indiana) migrates to Corepoint Health’s Integration Engine.
For $199, you can purchase a new genetic test that predicts the risk of male and female hair loss. Though I personally would hate to lose my hair, I’m quite fond of bald men, so I wonder why a guy would waste this kind of money? I suppose the idea is that if you are going to go bald, you can take medications early to slow the hair loss, though apparently the meds include a threat of “sexual” side effects. Men: bald is sexy.
Ambulatory surgery center operator AmSurg selects ProVation MD software by Wolters Kluwer Health.
A new P4P survey reports that P4P payments have grown to over 7% of physicians’ total compensation and 4% of hospitals, with some physician programs producing 30% of physicians’ compensation. Since 2006, the percentage of programs reporting quality improvements due to P4P has doubled and more than half of P4P programs cite measurable increases in their providers’ clinical quality.
The Alaska Native Tribal Health Consortium awards GCI $250,000 to provide a statewide broadband network to give health care provides more ready access to patients’ EHR.
WestCare Health System (NC) implements Preferred Medical Marketing’s Estimator PRO software to provide patients written estimates for expected payments due.
The Michigan Health & Hospital Association commits to a three year contract with ECRI Institute Patient Safety for ECRI to provide support for the Association’s patient safety data collection and analysis project.
Residents strolling their Aurora, CO neighborhood find personal medical documents littering their streets. Apparently the “trash” came from a healthcare facility eight miles away and included names, addresses, social security numbers, and other personal data. The healthcare facility is uncertain how the papers got there and is investigating.
Finally, a San Diego State University study finds that there are more indoor tanning salons than either Starbucks or McDonalds. Did my tax dollars help pay for that study?















































The news about AHRQ is very unfortunate. The AHRQ staff were always excellent to collaborate with. They had an impressive…