

News 2/11/09
From Brailer’s Revenge: "Re: another non-profit seeking hospital and vendor members. Most hospitals would have to ante up $8-20K for a seat at the table. Not clear what you get in return." Link. The National eHealth Collaborative’s initiatives include prioritizing standards initiatives and NHIN (it’s the AHIC successor, as it was known for awhile). It was just launched last month and John Glaser (who’s on its board) described it right here on HIStalk right after that. It’s a pretty big deal, especially with stimulus money coming and some structure needed around it, and entirely above board. I don’t know why hospitals would join either, but if they’re spending big money on EHRs, they at least get some voice in long-term direction. And, coincidentally, right after I wrote this, I got an e-mail from NeHC communications director Meryt, who sent over a newly released white paper developed with HITSP and CCHIT (fulltext on John Halamka’s blog, which saves me having to post it) that lays out their vision.
From Ex IBM’er: "Re: Healthcare and Life Sciences. Several folks RIF’ed out today."
From The PACS Designer: "Re: Alfresco. Enterprise Content Management is becoming more in demand by healthcare professionals and one free software solution addressing ECM is called Alfresco. HIStalk sponsor Red Hat has some experience with being an Alfresco installer and can help those who are interested in this software solution." Link.
From Cloud Jumper: "Re: alternative to HIMSS. Maybe you could do something like the TED talks, where the coolest people could give their talks to cool savvy people in the audience and it’s all on video so we can watch it later if we were uncool enough not to be invited. You could get the vendors to do tasteful little ads in front of each video, as TED does, to pay for it." That would be fun, although healthcare is so profit-oriented and fiercely protective of turf even on the non-profit side that the cool factor is turned down several notches (kind of like being the heppest cat at HFMA). Still, it would definitely be different than the mainstream conferences, where the same old faces exaggerate their successes with the same old ideas prettied up to seem more daring and contemporary. But, the one article commenter was spot on: HIMSS can only put people on stage who volunteer to be there, so those who have never been a speaker or committee member have no excuse to gripe about the result (I have, so I can). That’s one of my HIStalk goals, though — to showcase the good ideas of people who don’t have the time, money, or ego needed to ride the PowerPoint Podium.
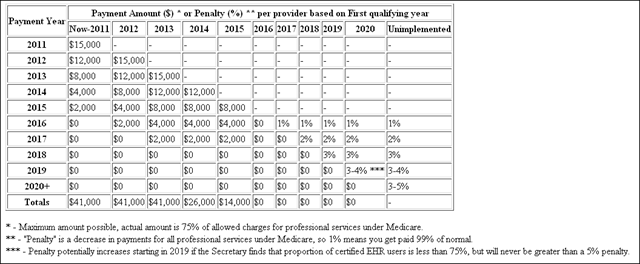
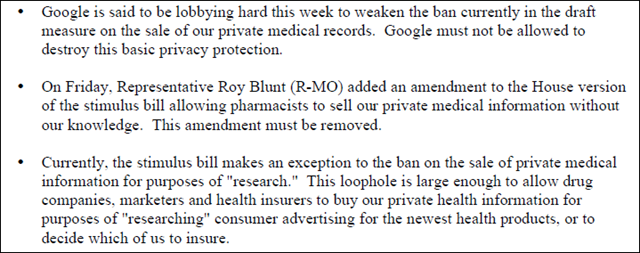
The Senate passes the economic stimulus package and Kaiser Family Foundation has a summary of it (the current version, until a compromise is reached with the House). The Senate’s bill calls for $19 billion for HIT vs. $20 billion in the House bill. Both sides want to give Rob Kolodner’s previously shoestring-funded office incomprehensible amounts of "discretionary" funds, $3 billion vs. $2 billion (is anyone a little scared of that?) Surely up for heated debate: the Senate’s bill punts on privacy, while the House calls for strict privacy protections. Wall Street wasn’t exactly overjoyed with the grim reality of this financial Hail Mary or the worse-by-the-day bank bailout; the major indices all dropped nearly 5% on Tuesday.
Speaking of that, the former lieutenant governor of New York weighs in with Ruin Your Health With The Obama Stimulus Plan. She says senators should vote against what she calls "the handiwork of Tom Daschle": ONCHIT as a big new bureaucracy, government interference with physician decisions, and intentionally slowed development of new drugs and technologies because they’re expensive. Daschle, she says, thought seniors should deal with conditions that come with old age instead of being treated for them, moving dollars to younger people (as cold as that sounds, I’d have to agree at least in general). Here’s the big finish: "The health-care industry is the largest employer in the U.S. It produces almost 17 percent of the nation’s gross domestic product. Yet the bill treats health care the way European governments do: as a cost problem instead of a growth industry. Imagine limiting growth and innovation in the electronics or auto industry during this downturn. This stimulus is dangerous to your health and the economy."
Add Rush Limbaugh to the list of HITECH haters. From his Monday show: "Your medical treatments will be tracked electronically by a federal system. Now there are arguments back and forth about whether or not this is a good thing. The opportunity for the loss of privacy is huge here … by digitizing and making everybody’s healthcare records computerized … especially having a major federal database where everybody’s health records are." I’m conservative and even I can’t stand that pompous gasbag, so I can’t imagine who’s still listening to him.
The New York Times just published a piece on HITECH, citing a letter that urges not just throwing EHR money at doctors, but also distributing lessons learned via "Regional Health IT Extension Centers" to help out with projects in small medical practices, which sounds like a great idea. You will note that the letter (warning: PDF) has few vendor signatories, unsurprisingly.
Cerner’s Q4 numbers, announced after the market close: revenue up 18%, EPS $0.86 vs. $0.49, thrashing expectations of $0.59. Say what you want about good old Republican boot-strapper and plain-speaking Neal, but the man knows how to run a company better than those big, fancy foreign conglomerates choking on healthcare IT and everything else they toe-dip into. Thank goodness for MEDITECH, Cerner, and Epic, run by the founders instead of hired gun Wall Streeters and sticking to their healthcare IT knitting instead of selling nuclear weapons, theme parks, and jet engines (not to mention toxic assets to taxpayers in one huGE example).
I got a couple of e-mails suggesting that Medical Records Institute, the folks who run TEPR, have laid everyone off and closed down. I’m sure that’s somehow tied in with their new focus and conference, but perhaps the change was more severe than was hinted. I’m sure updates will follow.
Listening: Seether, South African metallish grunge.
IBA/iSoft gets two contract extensions with Netherlands hospitals.
A surgeon in Australia develops a USB emergency button that, when pressed, sends a message to all PCs on the network along with the location of the sender. He created it after noting that several doctors had been killed by patients.
Allscripts announces that it will sell its Medication Services business (I asked Glen Tullman about it almost three years ago). The company also approved a $150 million stock repurchase plan.
Hospital layoffs: Columbia St. Mary’s (WI), 54; Cascade Healthcare Community (OR), 74.
Jobs: FCP-MS4 Patient Accounting Expert, McKesson Horizon Lab Consultant, IT Director.
Healthcare Growth Partners publishes its Q4 2008 Healthcare IT Transaction Summary & 2008 Year in Review (warning: PDF).
IBM and UnitedHealth test the medical home model, in which a primary care physician (not a gatekeeper) coordinates care among other medical professionals, often by using information technology. I’ll defer to Scott Shreeve, who provides a better synopsis than I can.
Interesting: hospitals that hire doctors often write employment contracts that don’t allow the doctor to contact patients if he or she leaves and also prohibits them from opening a practice within a specified radius. Patient are also charged large amounts to have their paper records copied so they can seek care elsewhere. Noncompetes are standard in business, in case nobody noticed that even non-profit healthcare is one.
A third of Australian healthcare and IT professionals say they’ve experienced compromised patient safety due to IT downtime.
Idiotic lawsuit: an admitted alcoholic on a two-day bender (more like a "breaker" in this case) in a Marriott falls more than 100 feet off a stairway while drunk, causing what he says is permanent brain damage. He’s suing the hotel for serving alcohol to an addict (him) and thereby causing his injury. He’s claiming injury, pain and suffering, anguish, disfigurement, medical expenses, loss of earnings, loss of the enjoyment of life, and aggravation of a previous condition.
A laptop stolen from Parkland Hospital (TX) last week may contain information on over 9,000 employees.
Availity announces the availability of real-time Florida Medicaid eligibility and claims status at no charge.
HERtalk by Inga
From Ronald Miller: ”Re: Henry Schein. Former MED3OOO VP Keith Slater is now the GM at Henry Schein Medical Systems. Good move for Henry Schein. It was only a matter of time until they figured out they had NO CLUE how to deal with a PM/EMR product after spending all that money on it. Maybe now the button ups at Schein will do a better job than Pfizer did with Amicore.”
From Jerry McGuire: “Re: Great piece today with Allscripts CEO on stimulus. From your piece, it seems the curious angle is identifying when IT does and doesn’t serve as a stimulate function. Maybe a virtual roundtable?” We’d love to hear readers’ opinions on what IT functions could stimulate the economy.
The Washington Post posts a graphic that breaks down the $819 billion stimulus package. It doesn’t say where the $20.2 billion for HIT is going, much less what part of IT is stimulating, but it is a pretty impressive graphic.
Caritas Healthcare (NY) files for Chapter 11 bankruptcy protection and its two hospitals are projected to close this month. Caritas had a net loss of $64 million for 2008, prompting the board to vote to close Mary Immaculate and St. John’s Queens hospitals.
QuadraMed announces that revenue for FY08 will be slightly ahead of the $146-149 million guidance previously provided. The company also expects EBITDA to significantly exceed the previous $15.8 million target. Reading between the lines in the press release, Keith Hagen sounds a bit cautious when discussing 2009 and the company’s potential for new business: “Approximately two-thirds of our revenues are produced by recurring maintenance and term license contracts, and a large percentage of our 2009 revenue is expected to be generated by this recurring base, our project backlog, and our broad set of products and services."
The 25-bed Hiawatha Community Hospital (KS) becomes the 55th hospital to go live on IntelliDOT’s BMA system.

Catholic Health Initiatives names Michael O’Rourke its permanent CIO and senior VP. He’s been interim CIO since August 2008 for the 77-hospital organization.
Capsule announces that 10 new healthcare organizations selected its device connectivity solution during the last quarter of 2008.
Marshfield Clinic (WI) adopts a new BI solution to make better use of its vast amount of patient data. Marshfield will utilize SAP’s Business Objects XI intelligence system to improve patient care and analyze internal business operations.
Eclipsys announces that Greenwood Pediatrics (CO) has selected Eclipsys PeakPractice (the former Medinotes PM/EHR solution). The 10-physician group apparently chose Eclipsys over Epic, which their hospital offered to subsidize.
A former Queen’s Medical Center (HI) administrator pleads guilty in federal court for defrauding her former employer out of $594,000. Patricia Syling is accused of creating bogus contracts between a company she owned and Queen’s, and charging the hospital for services that were not performed. Syling was hired by Queen’s in September 2001 as the corporate compliance administrator and director of revenue cycle. In an unrelated charge, Syling is also accused of defrauding another former employer, Citrus Health Care of Florida, of more than $1 million and using $320,000 of the proceeds to buy a luxury sky box at Tampa Bay Buccaneer football games.
The McKesson Foundation awards $60,000 in grants to nine Minneapolis-St. Paul-area non-profits. The funds will be used to support health and wellness programs benefiting children and families.
A Texas Medical Association survey finds that doctors worry their financial hardships threaten quality of care and access. Declining payments, claim denials, incorrect or late payments, and administrative burdens are taking time away from patients.
The University of Chicago Medical Center (the First Lady’s old haunt) plans to cut 450 jobs in order to cut 7% off its annual budget. This is in addition to the elimination of 15 senior executive posts, including the one vacated by Michelle Obama (we’ll try not to be cynical about the huge raise UC gave her just before Obama won using the rationale that she was essential and therefore worth every penny).
MRO expands its services to include remote release-of-information processing and remote and staffed services.
HIMSS Analytics releases a list of the top vendors of acute care EHR systems based on total number of installations. For 2008, MEDITECH topped the list at 26.6%, followed by McKesson (14.1%) and Cerner (12.6%). I wonder how the rankings would end up if the list were based on number of total beds?
The octuplet story just gets crazier and crazier. Apparently the mom’s fertility doctor is not as successful as most doctors around the country, with his patients having much lower than average rates of pregnancies and births. Also, at least two former employees have sued him, including an office administrator who accused Kamrava of tax and insurance fraud. The office manager claims the office kept two sets of books, one for cash and the other for insurance, and some cash was never entered into the computer or deposited in the bank. Meanwhile the Kaiser Permanente hospital where the children are receiving medical care is requesting Medi-Cal funding to help pay for the octuplets’ medical care since Mom is unemployed, living on food stamps, and mostly letting her mother raise her first six children.
Compuware’s Covisint subsidiary collaborates with the VIP Health Initiative to provide a secure single point of access to share clinical data. The VIP Health Initiative was formed by Scripps Mercy Physician Partners, SMPP Services and Physician Partners Management Services.
Despite massive financial losses as a result of Hurricane Ike, UTMB Galveston intended to pay $3 million in bonuses until a faculty group discovered the plan. According to the Texas Faculty Association, once the bonus plan was uncovered, UTMB canceled the payments. The largest bonus recipient would have been the school’s executive VP, provost, and dean of medicine, who was scheduled to receive over $122,000 – on top of his $700,000 annual salary. The school claims it was planning to cancel the bonuses anyway.
































Thank you for the mention, Dr. Jayne — we appreciate the callout, the kind words and learning more about the…