From The PACS Designer: "Re: digitally connected patient. TPD last year made HIStalkers aware of a new method being developed to capture patient information from remote locations. The first applications were seen in ambulances where patient info was sent to the hospital while transporting the patient. The Digitally Connected Patient or DCP provides caregivers with information about the patient’s condition and warns when conditions change that can cause harm to the patient. Now, the Cleveland Clinic Foundation has partnered with Microsoft on a pilot study to send patient data from the home to the hospital’s eCleveland Clinic MyChart and then to HealthVault to provide a more complete PHR of the patient experience." Link.
From A CSC Executive: "Re: NPfIT. You mentioned that CSC, Accenture, and Fujitsu slunk away from NPfIT. Could you update the note to remove the CSC? As the article mentions, CSC is still one of the major contractors and we took over additional responsibility when we picked up Accenture’s regions." My apologies. I’ve corrected that slip-up. Accenture and Fujitsu bailed out, but CSC is running a big piece of the project and not complaining about it as far as I know.
From Doogie Howitzer: "Re: Digital HealthCare & Productivity. It’s going down the tubes after two more issues." I can’t say I’ve ever read it either online or on paper, but maybe someone will miss it.

From Lou Loomis: "Re: Microsoft. In reference to your news on 11/7 about Microsoft, the attached was taken last weekend in Toronto. Several of us watched as the billboard operator added some patches to his Windows PC, rebooted, and then started the billboard software again. For reference, this billboard was about 3 stories high!!"
From Ouch: "Re: MEDITECH’s financials." Link. Q3 revenue was up, but net income went from a $27 million gain to a $21 million loss as the company wrote off $50 million worth of investment securities with permanently impaired value (maybe someone who was better in accounting class can help me interpret their numbers, which seem to look good other than the investment hit).
From FormerCT: "Re: layoff. Heard that HealthPort, formerely Companion Technologies, recently held another round of layoffs, its second since August, in an effort to improve the bottom line. The investors paid $40 million to buy Companion from Blue Cross and are having trouble turning a profit, let alone a return." Unverified.
From Stuck: "Re: Sage Healthcare. Mark Ryan, senior VP of customer services and support, has resigned." Unverified. He’s still on their Web page.
From Brother Windy: "Re: wherethemoneygoes.com. Any idea what happened to it?" The author of the site that railed against the financial excesses of non-profit hospitals, a caustic former Chicago reporter nicknamed Low Blow Joe, was outed as a paid shill for insurance big shot and health savings accounts advocate J. Patrick Rooney, who died in September. He also ran a vicious anti-Obama site for Rooney. Without Rooney’s paycheck, the site is apparently defunct.
From Wompa1: "Re: WHO report on world healthcare. This excellent analysis from The Cato Institute puts armchair musings to shame." Link (warning: PDF).
Proof that newspapers are not only getting skinnier, they’re also getting sloppier. This business journal story covers a local hospital’s EMR implementation, managing to (a) not give the hospital’s name except as ‘Harrison’ (it’s Harrison Medical Center); (b) not provide a location for either the hospital or the publication itself, except to say Kitsap (it’s in Bremerton, WA); and (c) not spell the vendor’s name correctly (Eclypsis instead of Eclipsys).
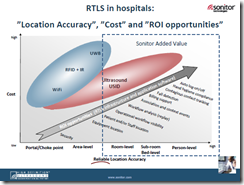
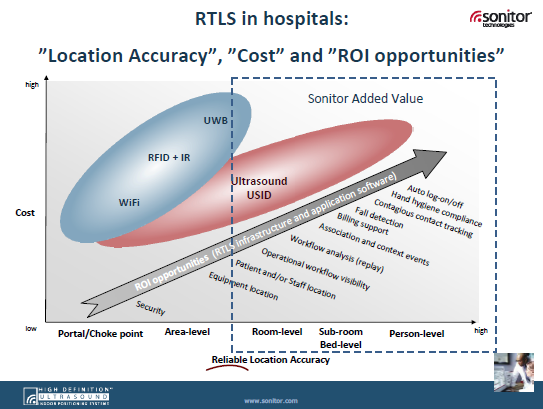
I mentioned that Sonitor was one of a handful of technologies that impressed me at HIMSS (disclaimer: they’re a sponsor now, but weren’t then). Anyway, I ran across the interesting slide above on RTLS opportunities from products like theirs.
I mentioned a few days back that I kind of liked Carol, "the Travelocity of healthcare," even though I’m totally unsold on all the brash consumer-driven healthcare startups trying to cash out before the bubble bursts again altruistically improve society’s health through consumer empowerment. Anyway, Carol cuts a fourth of its staff and changes its business model to focus on provider consulting and software, ditching the idea of letting consumers compare providers themselves. There’s $30 million in VC money shot to hell.
DR Systems claims it invented PACS and is going after other vendors, claiming patent infringement. Want to know what it costs to make them go away? Now you do: Emageon’s 10-Q says they paid DR Systems $1 million (it looks like a deal at $1,000 until you realize they’re omitting thousands).
Healthia Consulting, the force behind what some folks called the hottest event at HIMSS (the HIStalk party), will be rebranded under the Ingenix Consulting banner. Ingenix now has over 1,000 consultants from its several acquisitions and is serving providers, employers, insurers, pharma, and the public sector. Check out (and click) their new ad to your left to review their offerings.
The CEO and IT Director of 24-bed Eastern Plumas Health Care (CA) make a board pitch (unanimously approved) for a clinical system from Dairyland Healthcare Solutions (now called Healthland). Total cost with software, hardware, and implementation will be $322,500.
Scripps Health (CA) interim CIO Patric Thomas gets the job permanently.
Capsule announces 10 new DataCaptor medical device connectivity sales.
Patricia Lavely of Memorial University Medical Center is named CIO of the Year by the Georgia CIO Leadership Association.
Premise gets some big-name new customers for its patient flow solutions: Children’s Hospital Boston, Hospital for Special Surgery, and UCSF Medical Center.
IBA’s iSoft announces the launch of its Lorenzo system to the rest of the non-NPfIT world, taking shots at Cerner and other vendors in the press release. IBA says the potential market is in the billions and it expects to double revenue as a result.
The White Stone Group, which offers systems that document and track the business and clinical communications of hospitals, gets a nice profile in the Knoxville business paper.
The Longstreet Clinic, PC of Gainesville, GA wins a statewide e-Technology Award for its EMR implementation.
Catholic Health Initiatives will implement NCR’s MediKiosks to reduce patient wait time.
UPMC will use its patient database to create a voluntary registry for patients to be alerted about clinical trials.
The Wall Street Journal weighs in on ICD-10 in an article called Why We Need 1,170 Codes for Angioplasty. They seem to conclude that it’s cumbersome but probably necessary given the limits of ICD-9.
E-mail me.
HERtalk by Inga
From Lola Falana: “Re: HCIT funding. MDs could buck up and do CPOE. The now-tired ‘time is money’ excuse ignores that they have the equivalent of a gun in their hand with paper orders. They could come on board tomorrow at zero cost to them and get back the OE time with order sets, reduced calls, and other time-wasters. The culture is already changing with younger clinicians and increasingly onerous third-party, data-intensive reporting for compliance and reimbursement. I know MDs want subsidies, but let’s start with what we can do now with CPOE and Stark. We can adopt a patient safety culture without waiting for Barack. The whole country, including HCIT, needs change.” I agree that mandates may be the answer, though nominal penalties like 2% probably won’t be enough.
AARP, Business Roundtable, Service Employees Union, and National Federation of Independent Business send an open letter urging President-elect Obama and Congress to build on the SCHIP, to promote preventive care, and to advance HIT adoption. The four groups are part of an organization called Divided We Fail, aimed at promoting healthcare reform now.
A report concludes that excess installed capacity and initiatives to reduce health care costs will negatively affect sales of CT systems, MRI, and nuclear medicine scanners over the next five years.
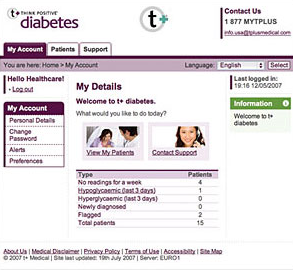
A study finds that when patients receive treatment alerts along with their physicians, compliance increases by 12.5%, with the greatest improvement in diagnostic recommendations.
St. David’s HealthCare (TX) blames the economic downturn on its decision to lay off 50 employees in non-bedside, non-patient care areas.
The Ventura County, CA newspaper reports that the local county clinic system had 44,000 more patients in the last year while hospital procedures are down about 9% over last year.
Another sign of the times: Starbucks reports a 97% fall in profit (and a 50% drop in stock price over the last year). I’m not sure I could carry on if I didn’t know I could find a Starbucks within a five-minute drive just about anywhere I am, so I hope Howard Schultz figures it out.
Amid pressure from clinical staff critical of his management style, Northeast Health Systems (MA) CEO Stephen Laverty resigns. According to the Wicked Local Gloucester (great name for a newspaper), Laverty was focused on advancing HIT at this 100 Top Hospital. During his eight-year tenure, the hospital implemented a number of new technologies, including PACS, CPOE, and voice recognition.
Biopharmaceutical company Favrille and PHR developer MyMedicalRecords announce a merger.
ACS gets a $44 million deal to provide business outsourcing services for Florida Medicaid. ACS will be tasked with helping the agency save money on Medicaid bills by identifying possible private insurers.
Doctors in California, Nevada, and Hawaii claim that Medicare is late in paying them millions of dollars. The problems stem from May’s changeover to UPINs and September switch to a new claims processor.
E-mail Inga.
Veterans Day
Freedom is not free – thank a soldier or veteran and remember those who have given their lives. If you’re a veteran, on active duty, or serving in the reserves or National Guard, thank you.

In Flanders Fields
By John McCrae
In Flanders Fields the poppies blow
Between the crosses row on row
That mark our place; and in the sky
The larks, still bravely singing, fly
Scarce heard amid the guns below.
We are the Dead. Short days ago
We lived, felt dawn, saw sunset glow,
Loved and were loved, and now we lie
In Flanders fields.
Take up our quarrel with the foe:
To you from failing hands we throw
The torch; be yours to hold it high.
If ye break faith with us who die
We shall not sleep, though poppies grow
In Flanders fields.
Help a Wounded Veteran Recover
I like to think my problems are important, but only until I remember those soldiers who are coming back from terrible struggles in Iraq, Afghanistan, and other far-flung parts of the world. Kids are coming home horribly maimed and disfigured before they even had a chance to experience normal adult life. Despite their ruinous injuries, they might even consider themselves lucky because, unlike some of their fellow soldiers, they made it back.
I was struck today when I accidentally ran across Project Valour-IT, which is run by Soldiers’ Angels. The nonprofit group’s motto is, "May No Soldier Go Unloved." The project, originally named as Voice-Activated Laptops for OUR Injured Troops, supports severely wounded soldiers by providing them with voice-controlled laptops, whole-body video games for physical therapy rehabilitation, and personal GPS devices to help them relearn mobility with their impairments and physical challenges.
Donations go 100% toward the laptops – nobody in Soldiers’ Angels gets paid. They received this from a grateful soldier: "To Whom It May Concern, Hello, my name is LCpl. Andrew. I am a Marine that was wounded in Iraq and got medevaced to Brooke Army Medical Center in Ft. Sam Houston, Texas. I recently received a laptop. I was informed that it was you, the Soldier’s Angels that donated it. I can’t tell you how thankful I am to have support from organizations such as yourself. It really lets me know that there are people out there that still care about the troops and what they are sacrificing for this country. I appreciate what you have done for me and having this laptop is actually good therapy for my hand. Once again thank you and I am proud to serve this country knowing there are people like you that I am protecting. Sincerely, Andrew."
I was moved to do two things today. First, I donated $800 (anonymously), the amount needed to fully fund a soldier’s laptop. I spoke to the founder and she assures me it will be put to great use in one of the military hospitals. In fact, she invited me to visit either Bethesda or Brooke Army Medical Center to present it myself. If you want to donate that tax-deductible amount, you are also welcome to correspond or visit the recipient to encourage his or her recovery through moral support. They get a great deal from Best Buy on state-of-the-art laptops with all the assistive technology installed, ready for immediate use (she wanted me to thank Nuance for helping them out in the past with Dragon Naturally Speaking discounts, so here’s a shout out to them).
Second, Project Valour-IT is running a blog contest from now (Veterans Day) until Thanksgiving. You can donate any amount to help the cause. Donations aren’t tracked by blog, but rather by teams representing each military branch (it’s actually just for fun since all the money goes into the same pool, but it does spark friendly rivalries). I chose the Navy Team because: (a) I have been to Navy football games and the Midshipmen are the most disciplined and respectful students I’ve ever seen; (b) I will argue passionately that the Naval Academy is not only the most beautiful campus in the country, but is also in the top handful of colleges academically and competitively and maybe #1 when you count leadership; (c) Mrs. HIStalk’s father was a Marine; and (d) I can say I know a Navy Rear Admiral, Cindy Dullea of SCI Solutions. OK, it’s sketchy logic, but I had to pick one of the branches, so there you go.

If you would like to help Project Valour-IT, click the fundraising graphic I put up on your right, which will take you to a donation screen. Donate $250 or more and you’ll get a special gift. And, since I can’t see the donations and they aren’t tracked separately for HIStalk, please post a comment on this article (click the Comments link at the bottom) and just mention that you helped them out. Thank you for your support.






























































{kind=link}
The news about AHRQ is very unfortunate. The AHRQ staff were always excellent to collaborate with. They had an impressive…