

Monday Morning Update 9/3/12

From HITEsq: “Re: McKesson. Won its appeal against Epic for patent infringement. The Federal Circuit, en banc (i.e., before all the court of appeals judges), overturned existing law to find in favor of McKesson. The case is remanded to the lower court to decide if Epic really does infringe.” It’s a complex issue, and since I covered it when McKesson lost the original appeal in April 2011, I’ll recap from there. McKesson said Epic’s MyChart violates a McKesson patent for a method of placing visit-specific patient information on a Web page so that patients can schedule appointments and request prescription refills. The original “joint infringement” decision (about which the three-judge panel argued a lot) was that Epic wasn’t liable since it doesn’t directly offer those capabilities, but rather allows individual patients to request MyChart access subject to the approval of their physician. Since no single party violated McKesson’s patent, the original court said Epic wasn’t liable. Legal experts are troubled with this latest decision, which appears to make “inducing infringement” actionable even if no infringement has been proven. All of this is way over the heads of mere non-lawyer mortals like myself who can’t resist snickering while repeating phrases from the document like “joint tort feasor” in humorous voices because it’s just so weird and funny, so if any legal beagles wish to expound pro bono, here is your electronic lectern.
Patent on personally controlled health record with notation of source/ authority (filed 3 yrs ago) HT
@craigjoseph patft.uspto.gov/netacgi/nph-Pa…”— Farzad Mostashari (@Farzad_ONC) August 31, 2012
From Lex Luther Van Dam: “Re: Epic’s patent for a patient-controlled, patient-generated health record. This is bizarre. Much of this was already on the market when the patent was filed, so either Epic didn’t know or forged ahead anyway, and either is not good. Epic has seemed indifferent to patients controlling their own information, to the point that they don’t even talk about Lucy, their own PHR solution, and they certainly don’t cooperate with anyone else offering a PHR solution.” My guess is that this patent either covered Lucy when it was first being developed or was simply a legal stake in the ground to prevent further legal incidents like the McKesson one above. I also don’t know that Epic’s customers, being turf-protecting and somewhat patient-paternalistic academic medical centers, have a heartfelt interest in empowering their patients via PHRs from Epic or anyone else. Or for that matter, avoiding the “walled gardens” between proprietary EMRs that Farzad was railing against given that Epic-to-Epic direct data exchange has displaced the interest in a vendor-neutral exchange in some areas where most of the major players run Epic.
From MU Nick: “Re: worksheet. Has anyone created a worksheet for MU2 for the EP and EH requirements (as opposed to a PDF?)” If you’ve put something together and are willing to share, let me know.

From DanburyWhaler: “Re: Western Connecticut Health Network. Hired Steve Laskarzewski, Waterbury’s former CIO, as clinical applications director. Looks like they’re grooming him for the top spot when Kathy DeMatteo steps down later this year.” Steve’s LinkedIn profile says he started in June. He’s one of the 2,716 members of the HIStalk Fan Club that reader Dann started years ago, so he gets a shout out.
From Douglas: “Re: Mr. HIStalk. Why do you use that name?” I needed an e-mail address when I started HIStalk back in 2003, and being in a minimally creative mood at that moment, the best I could come up with was mr_histalk (the name HIStalk itself was equally lame, with the HIS standing for Hospital Information System, which was in vogue at the time). I had zero readers and minimal expectation of gaining any, so I didn’t give it much thought. I don’t recall having actually called myself that at any point, but readers did over time, and then Inga at some point shortened it to Mr. H. It feels odd since I have never even once referred to myself as Mr. Anything in real life since I’m not too impressed with titles in general. My latest pet peeve: family members of dead doctors who stick “Dr.” in the title of their obituary listing instead of just their name like everybody else does, apparently hoping that like Egyptian boy kings, their most valued earthly possession will carry over into the afterlife. Putting “MD” after your name is perfectly fine on your office door, as is “Doctor” in front of your name is for professional encounters. A doctor who is so deficient in self-esteem as to demand the use of those titles in social situations when nobody else is calling themselves Mr. or Ms. is, in my opinion and experience, an arrogant ass. Lots of people earn doctorates, many of them requiring more education than a medical degree, and yet it’s most often an MD (or, in the case of male MDs, their wife) who insists on cramming their title down everybody’s throat at the auto repair place or at school meetings (my theory: that’s why hospital administrators enjoy putting physicians in their place). So, to complete my circular logic, the Mr. HIStalk thing is not indicative of a superiority complex since if anything, my tendency is the opposite.
It’s Labor Day, so I am appropriately laboring (in the non-obstetrical sense). I hope your holiday is – or was, depending on when you’re reading – delightful.

We are collectively fatigued with the endless Meaningful Use palavering, apparently, as 46% of respondents say they are indifferent to release of the Stage 2 rules. Of those who cared, reaction was split between positive and negative. New poll to your right: if the presidential election were being held today, who would you vote for? An online issues quiz says that I’m exactly evenly split between the two major candidates with a 63% alignment with my beliefs for each, but both are far dwarfed by my 91% match with Libertarian candidate Gary Johnson, who I’d never heard of until I took the quiz. That leaves the same options I had in the last presidential election: vote for either of two candidates that I would dread seeing take office or vote for one I’d like to see win who doesn’t have a chance.
![]()
Surescripts acquires Kryptiq, of which it previously owned a 21% share. Surescripts uses Kryptiq’s secure messaging technology for its network. Other healthcare IT vendors are also among its customers (GE Healthcare and Vitera), and its other offerings include clinical messaging, a patient portal, and electronic prescribing. Kryptiq announced earlier this year that its revenue grew 60% and its user count exceeded 40,000.
Cambridge Health Alliance chooses EDCO’s Solcom electronic document management system for managing historical paper records and paper documents originating outside of CHA. It will integrate that information with its Meditech and Epic systems to eliminate the file room and hybrid record environment.

Joint Township District Memorial Hospital (OH) chooses the Optimum general accounting suite from NTT Data. The company also announces that its NetSolutions Point-of-Care clinical and billing system for long-term care facilities will now send care data toAssured Proactive Analytics to optimize payment.

A Wells Fargo Securities report sent over by a couple of readers says that hospital users of Meditech, Cerner, and CPSI lead the pack in total number of Meaningful Use attestations through June 30. On the ambulatory EHR side, it’s Epic, Allscripts, and eClinical Works, although Epic would drop to third if it didn’t have 10,000 Kaiser doctors of its 15,000 attestations. Of new attestations, it’s Cerner and CPSI leading for hospitals (those same two vendors also led in the overall percentage of client base attesting) and athenahealth and Practice Fusion for EPs. A reader, however, notes that the numbers suggest that Epic has 650 hospital customers, which seems awfully high, so there’s always the question of what’s behind the data.

CoCentrix hires Clayton Ramsey (Elsevier) as SVP of delivery.
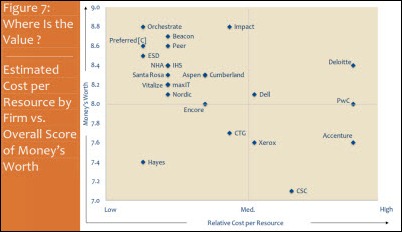
I chose this graphic in mentioning the new KLAS evaluation of Meaningful Use consulting firms a few days ago and regretted it the next day when I had more time to ruminate on it. I’m unhappy with how KLAS presented the graphic since they committed the cardinal sin of not setting the Y-axis of the graph to zero. That’s usually a red flag indicating that someone is trying to make an overly dramatic point that their data points don’t support. In this case, the actual range of consulting firm “money’s worth” scores was 7.1 to 8.8, which are pretty good numbers within a fairly narrow spread. The KLAS graph only shows the range of 7.0 to 9.0, making it appear that huge gaps separate the firms, which is absolutely not the case. This doesn’t give me a lot of confidence that the behind-the-scenes work at KLAS is statistically rigorous, a often-made but never-answered charge. I would also question whether this graphic means anything at all considering that the Y-axis is customer-reported value, while the X-axis is “relative cost per resource,” whatever that means. Should we infer that a company with a high per-resource cost can’t be worth it no matter how satisfied their customers are? My main gripes with KLAS (and the Most Wired surveys and HIMSS Analytics and so on ) is their tendency to take a modest amount of data and over-extend it to lofty conclusions using a black box that nobody’s allowed to peer into. I like what they do, but as we healthcare types say, “In God we trust – everybody else bring data.”

Among the speakers at this past weekend’s health IT conference in Hyderabad, India were Lee Shapiro (Allscripts president) and Marc Probst (Intermountain Healthcare CIO).

TeraRecon launches its iNtuition Review, iNtuition Enterprise Medical Viewer, and iNtuition SHARE at the AOCR/RANZCR radiology conference in Sydney, Australia. The products provide multi-modality review and the capability to distribute images throughout the enterprise via a browser-based viewer.

Cancer Care Group (IN) announces that medical information of 55,000 patients and the organization’s own employees was exposed when server backups were stolen from an employee’s locked car. The announcement leads off with, “Patient confidentiality is a top priority,” which is apparently now a bit closer to the truth since they’re suddenly considering encrypting backups and mobile devices. It’s an immutable rule that nobody encrypts anything until they are publicly embarrassed for not having done so, and then they can’t jump on board fast enough.

Novant Health (NC) rolls out a screensaver featuring former UNC star Michael Jordan to remind employees of its zero-tolerance handwashing program, launched in 2005 after three premature babies died in one of its hospitals from MRSA infection. The source was tracked back to staff who hadn’t washed their hands, which Novant found was common with a compliance rate of only 49%. They’re at 98% now.
In Australia, a hospital CEO sues a nurse who he says disparaged him in her Facebook comments that were brought on by a labor dispute. One of her comments: “We don’t take kindly to misinformation by well-paid fat cats who only visit the hospital wards for photo opportunities.”

Surgeon and best-selling author Atul Gawande, one of the most visible and respected people in healthcare, apparently is sold on the use of analytics but isn’t a fan of using technology in his own practice. Some snips from a recent interview:
- I do use the iPad here and there, but it’s not readily part of the way I can manage the clinic. I would have to put in a lot of effort for me to make it actually useful in my clinic. For example, I need to be able to switch between radiology scans and past records … I haven’t found a better way than paper, honestly. I can flip between screens on my iPad, but it’s too slow and distracting, and it doesn’t let me talk to the patient.
- I think that information technology is a tool in that, but fundamentally you’re talking about making teams that can go from being disconnected cowboys in care to pit crews that actually work together toward solving a problem.
- I worry the most about a disconnect between the people who have to use the information and technology and tools, and the people who make them. We see this in the consumer world. Fundamentally, there is not a single [health] application that is remotely like my iPod, which is instantly usable … In many of the companies that have some of the dominant systems out there, I don’t see signs that that’s necessarily going to get any better.
- The reason [data analytics] works well for the police is not just because you have a bunch of data geeks who are poking at the data and finding interesting things. It’s because they’re paired with people who are responsible for responding to crime, and above all, reducing crime … That’s what’s been missing in health care. We have not married the people who have the data with people who feel responsible for achieving better results at lower costs.
- Timeliness, I think, is one of the under-recognized but fundamentally powerful aspects because we sometimes over prioritize the comprehensiveness of data and then it’s a year old, which doesn’t make it all that useful. Having data that tells you something that happened this week, that’s transformative.
More on Keane’s HIS-tory this week from Vince.






































































































Anything related to defense will need to go to Genesis.