Top News

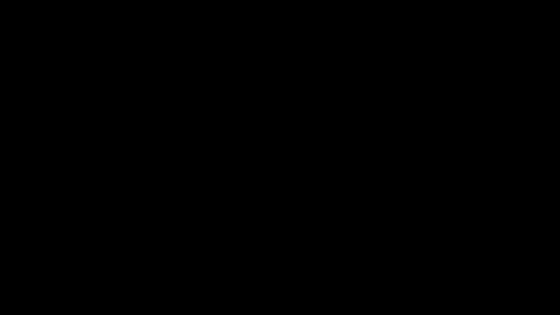
Nuance shares jumped 8 percent Tuesday after activist investor Carl Icahn disclosed that he holds a 9.3 percent stake in the company, with speculation that Icahn’s history of forcing underperforming companies to change may mean that he will seek to break Nuance into separate businesses. Above is the one-year share price (blue) compared to the Nasdaq (red).
Reader Comments

From Sequester: “Re: Vanderbilt University Medical Center. Sequester and Medicaid expansion hits the budget.” VUMC implements a hiring freeze for non-patient care positions, urges employees to control food and travel costs, stops vacation accruals through June 30, cancels the scheduled July 1 merit increases, and eliminate this year’s incentive bonuses. They need to make up a $20 million shortfall by June 30 and then find $50 million in ongoing annual savings.
From Hodor: “Re: HIMSS Analytics. We received an open records request stating we have to supply a copy of the contract with our EHR vendor as well as proposals from all bidders. This just seems wrong to me. A contract negotiated in good faith is now part of open records. Once we pick a vendor, we work at making it a partnership and this goes against all of that. I am seriously considering dropping my HIMSS membership.” Sunshine laws require that public organizations make their agreements available and I think hospitals are treated no differently than any other public agency or charity even though they often don’t think of themselves that way.
HIStalk Announcements and Requests
March easily set the record for one-month HIStalk readership with 156,337 visits, 266,440 page views, and 30, 824 unique readers. The needle pegged during HIMSS week with around 11,000 visits each day on Monday and Tuesday of that week.
Acquisitions, Funding, Business, and Stock

Emdeon announces its intention to re-price its existing senior secured credit facilities to benefit from current market interest rates.

Merge Healthcare announces a tender offer for all of the $252 million in 11.75 percent Senior Secured Notes that are due in 2015, hoping to refinance at a lower rate.

Colorado Governor John Hickenlooper joins TriZetto Chairman and CEO Trace Devanny in the cutting the ribbon for the company’s new headquarter in Douglas County, CO.
Sales
The Delaware Health Information Network will implement Audacious Inquiry’s Encounter Notification Service to alert physicians of patient admissions and discharges.

St. Francis Hospital and Medical Center (CT) signs a five-year contract extension for Streamline Health’s AccessAnyWare and FolderView suites and adds integration with Epic.
Rocky Mountain Health Plans (CO) contracts with HealthSparq for self-service websites for its insurance members.
People

NaviNet names Daniel Timblin (BCBS TN) CFO.

Health Evolution Partners promotes David A. Smith (PSS World Medical) from senior operating partner to general partner of the firm’s Growth Buyout Fund.

RazorInsights hires Karl Kiss (Siemens) as VP of sales and marketing.

Carol Zierhoffer (Xerox) joins the MedAssets board of directors as head of the IT committee.

MedHOK appoints Lisa Slattery (Health First) chief quality and compliance officer.

Availity names Karin J. Lindgren (Reed Group Ltd.) SVP of legal and regulatory affairs and general counsel.

Edifecs hires Sam Muppalla (McKesson Health Solutions – above) as SVP of products and strategy, Vik Anantha (McKesson Health Solutions) as VP of financial management solutions, and Prabhu Ram (GE Healthcare) as VP of clinical solutions.

Mark Snow (RevSpring) is named SVP of business development and marketing of revenue cycle outsourcing vendor GeBBS Healthcare Solutions.

Stephen Schuckenbrock (Dell) is named president and CEO of Accretive Health, replacing Mary Tolan, who will move to board chair.
Announcements and Implementations
The Patient-Centered Outcomes Research Institutes names 84 appointees to its first four advisory panels.

Weirton Medical Center (WV) goes live on its $30 million Siemens Soarian EHR and Siemens MobileMD HIE platform.
HL7 makes its standards and select intellectual property available at no charge under licensing terms. The organization is also revising its membership model to include an expansion of free or discounted education programs and training, a help desk, and enhanced testing of individual expertise in HL7 development, training, and implementation.

Patient Privacy Rights publishes its Privacy Trust Framework, a set of 75 criteria for measuring how well IT systems protect data privacy and patient control.

ZirMed launches Patient Estimation, a Web-based solution to determine a patient’s financial responsibility prior to providing care or service.
Government and Politics
The Missouri Senate approves legislation requiring insurance companies to cover telemedicine services if the same services are covered for face-to-face doctor visits.

Rep. Jim Dermott (D-WA) asks HHS to consider renewing its safe harbor provision that allows hospitals to subsidize EHR technology for its affiliated physicians under the federal Anti-Kickback Statute. The provision is set to expire at the end of 2013.
Rep. Diane Lynn Black (R-TN) proposes legislation that would exempt solo physicians from MU penalties based on lack of capital and resources, as well as exempt physicians nearing retirement age. Other provisions would expand the definition of an Eligible Provider to include rural health providers and to allow certain providers to participate in specialty registries in lieu of reporting on quality measures.

CMS has paid $12.7 billion in MU payments through the end of February.
A petition urges the White House to force the Department of Defense to use the VA’s VistA system to save taxpayer dollars and ensure continuity of care of veterans.
Other
An article in The Wall Street Journal covers saving the cost of repeated image scans by sharing them. Mentioned is lifeIMAGE, which offers radiology practice connections to the federal funded Image Share platform

A fun April 1 phony EHR demo from pedatrics EMR vendor PCC includes the often-requested One-Click Charting enhancement as well as exporting patient information directly to Facebook and Twitter.

Epic sets the standard for self-parody in its April Fool’s home page makeover. The lead story claims the company will release its secret Kool-Aid formula to meet ONC transparency guidelines and also apparently pokes fun at CommonWell in saying that other vendors are working on their own versions that promise to be more interoperable. It also announces Pair Everywhere, which will use shared personal information (entered by SmartText, of course) and ICD-10 codes to identify “that perfect someone who also likes long walks on the beach, dancing in the rain, and monitoring readmission rates for at-risk heart attack patients.” The short blurb says MU3 will require providers to wear bow ties instead of traditional ones as an infection control standard, while my favorite says the company will change its name from Epic to EPIC since “no one gets it right anyway.”
Speaking of Epic, a local article highlights the companies being launched in the area by former Epic employees, which have created 400 jobs in the Madison area. Profiled are Nordic Consulting, Vonlay, BlueTree Network, CenterX, and Moxe Health. Epic’s headcount is now at 6,400, the article says, up 1,000 from a year ago.
Craigslist founder Craig Newmark weighs in on the VA’s disability claims backlog in a Huffington Post blog post. He seems sincere, but not particularly insightful.
A Medical College of Wisconsin cancer researcher is charged with stealing another doctor’s drug research, sending it off to China, and then trying to delete data from the college’s computer system to avoid detection. The researcher had been disciplined previously for storing lab data on his own computer. He’s been charged with economic espionage.
Sponsor Updates

- Carl Fleming of Impact Advisors will shave off his hair and beard at the company’s annual meeting on May 1, hoping to raise $3,000 for the St. Baldrick’s Foundation. He’s at $1,290 in donations so far.

- ESD celebrates its 23rd year in business this week with photos and a company history.
- MedAptus suggests ways to survive Medicare cuts from the sequester.
- Accent on Integration will participate in the International MUSE Conference May 28 in National Harbor, MD.
- Rebecca Saffert, product manager with Optum Health, hosts an April 25 Webinar on reducing readmissions through transitional case management.
- Iatric Systems offers a two-part guide on how to use technology to prepare and meet the deadlines for MU 2014.
- Gates Hospitalists (MO) secures PQRS incentive funds using Ingenious Med’s claim-based submission registry.
- Levi, Ray & Shoup is sponsoring the CIO Summit in Newport Beach, CA April 8-10.
- Crain’s Chicago Business names Deloitte the 12th best place to work in Chicago.
- Kareo answers the top five questions from a recent Webinar on practice marketing.
- SIS offers four tips to improving coordinated care in the OR.
- First Databank announces its 2013 FDB Customer Seminar November 6-8 in North Miami Beach.
Contacts
Mr. H, Inga, Dr. Jayne, Dr. Gregg, Lt. Dan, Dr. Travis.
More news: HIStalk Practice, HIStalk Connect.


















































The $50 billion Rural Health payout is welcome. In context, it's less than the total cost of the F22 raptor…