From Seattle: "Re: HIMSS. At the HIMSS Washington dinner last night, Dave Garets of HIMSS Analytics disclosed that he and others from HIMSS had been working with the Congressional Budget Office on the HIT proposal.They were asked what would it take to get all hospitals to Stage 4. Apparently the proposal includes both inpatient and ambulatory and will be a combination of grants, loans, and Medicare rewards, including up to $1 million in ‘reimbursements’ for systems already implemented. When the speakers panel discussed this, two of the four suggested that this was a lousy idea and seriously questioned why we should be reimbursing anyone. They suggested instead delaying ICD-10 or using the simpler Canadian version or simplifying claims and payments, also focusing on reducing provider time by eight hours a schedule using technology instead of just buying more technology." HIMSS Analytics shows that 95.7% of hospitals haven’t yet made it to Stage 4, which requires all ancillaries to be installed, CDR, controlled medical vocabulary, CDSS for both error checking and clinical protocols, clinical documentation, PACS in all areas, and CPOE (even though you only need one live floor to claim victory). Maybe someone should get the cost and outcomes stats from those who have since I doubt there’s a corresponding improvement. Using that logic, Detroit should be rewarded for buying new robotic welders as a way to create safer and better cars. Why not just pay them for making safer and better cars? Makes sense unless you sell robotic welders.
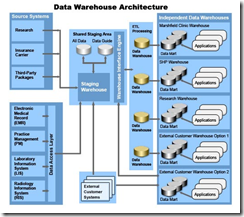
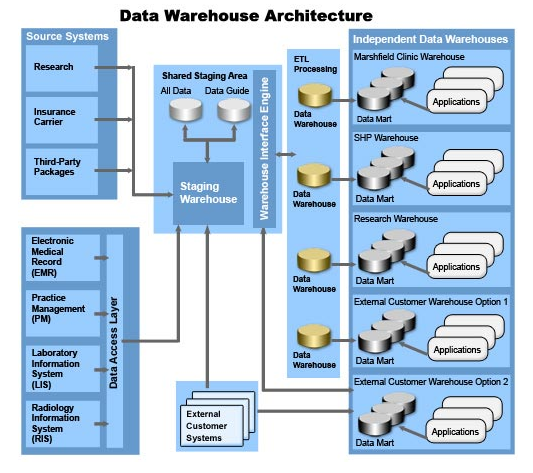
From Terry Jacks: "Re: Ministry. Is anyone going to point out that this Cattails system that has been recognized recently in the press is not a vendor, has no clients, no implementation staff, no service staff, and no customers other than their own docs? I thought we went away from home grown systems in the 1980s?" I think you may have given Pete inspiration for a future posting. From its data warehouse design above, it’s not exactly a stripped down, spur-of-the-moment system and it’s also CCHIT certified, so I’ll be interested to hear more about what they’ve built.
From Snake Pliskin: "Re: Sutter. The period of time that it has taken Sutter to implement Epic is NOT a reflection of Epic. Sutter is pushing the envelope. When you look at Epic, it’s pretty amazing to realize just what they have accomplished over the course of the past eight or nine years since they entered the inpatient arena. Sutter is a confederation that covers a huge geographical expanse. It’s been about establishing common governance, common processes, achieving consensus, responding to changes in technologies and patient care needs, the desire to improve work flows. I’m going to give Epic and Sutter kudos. Really. It’s a monumental task."
From Seattle: "Re: ICD-10. Compliance deadline extended to October 1, 2013." Link. AHIMA is "applauding" with its imaginary hands, but only for HHS’s approval of ICD-10. It’s not happy about the deadline extension. On the other hand, AHIMA doesn’t sell or use information systems, so that’s easy for them to say (good for coders, too, probably).

From Rommon: "Re: Palmetto Health Baptist Easley. The 50-year-old upstate SC hospital to be spun-off from the largest healthcare system in the state, Palmetto Health, and co-owned by PH and GHS. ‘Not related to the economy.’" Link.
From RIS Guy: "Re: Agfa. Agfa is, for the second time in four weeks, today going through a US reduction in force of about 60 people. This time, it’s front line sales and service."
From Billy Lyall: "Re: site visits. I have worked for vendors for much of my life and I’m always sensitive to site visits. They’re no easy thing to manage from the vendor perspective. They can be risky — even the best site visit could go downhill quickly. They consume a lot of time for the host. Of course the host is going to get something, maybe some discount on support hours or licensing of new products, but maybe even just special attention from the vendor. But, my impression of the people from the hosting site has always been that they are candid about support issues, implementation hurdles, staffing, and ability to meet end user needs. There’s always the opportunity for sidebar conversations." I enjoyed Ricky Roma’s piece and have asked for more if he’s willing. Inga and I found him by accident and were enthralled by his writing.

From Webbed_Feet: "Re: OHSU. Reorg and layoff alert; Oregon Health & Science University (OHSU) completely re-orgs IT. The final numbers are not published yet, but dozens have been told they will be laid off and will get formal notice on Wednesday. As part of the re-org, the CIO and CHIO formally announce the Clinical Informatics department that encompasses workflow analysis, clinical reporting, HIM nad RN and MD champions for the Epic project." OHSU has been struggling, so it’s probably not too surprising that something had to give.

From Medarling: "Re: Ivo Nelson. I heard interesting comments that Ivo Nelson, former CEO of Healthlink before selling to IBM, may be doing a comeback? Anyone else hearing this?" His LinkedIn profile indicates that he has started a new consulting business in Houston called Ivo Inc., which may or may not be just him puttering around a little. I finally found a personal e-mail address for him and sent an inquiry, but I haven’t heard back.
The House Appropriations Committee released a summary of its stimulus plan Thursday, which includes $20 billion for HIT. It will be interesting to see where the money would go once the details come out. Since Obama wants a quick jolt, the only reasonable way to disburse it would be through organizations that have been efficient and trustworthy in the past. How else, other than parachuting in pallets of cash a la Iraq, could that much money get into play quickly? Who would you trust to dispense it thoughtfully?
David Brailer writes his thoughts on the national health IT agenda, which unfortunately came out about six hours after I sent him a list of interview question and hoped for a response. He says he hoped to let the market drive EMR adoption when he was running ONCHIT, but it didn’t happen, so government incentives are needed. However, he nearly echoes my previous writings, I’m proud to say: "We should not incent physicians and hospitals simply to purchase electronic records. We get no benefit when a physician or hospital buys an electronic record. What we should do is reward the use of these tools as part of a patient’s care." He advocates pay for use. He also points out the obvious need for bunch of clinical informatics people to get all this stuff up and running, which of course is a hundred times harder because every vendor’s system is different and it takes years to really learn each one. He also suggest updating HIPAA and privacy rules, arguing that trusted providers are constrained while companies like Microsoft aren’t because they aren’t providers. Here’s his big pitch: "President-elect Obama should consider one single change that would do more to reshape medicine into an information industry than anything else: have Medicare treat electronic visits as equivalent to in-person visits." Brother Dave, this choirboy hears you loud and clear and says amen, although I might change that last big pitch to: "President-elect Obama should consider one single change that would do more to reshape medicine into an information industry than anything else: put a stop to all the ridiculous documentation requirements for getting providers paid, many of them imposed by Uncle Sam himself through his big payors like Medicare." Imagine how good EMRs would be if all the crap involving billing and malpractice defense could be eliminated and systems redesigned from scratch for the patient’s benefit, not that of the government and the insurance companies. It’s no surprise that the best clinical improvement came from the VA’s VistA – the hardhats didn’t have to program in that 80% of the average hospital system that has nothing to do with patients. Hospitals bought their first computers because of Medicare complexity and that hasn’t changed.
The chair of the House VA committee says he will investigate reported software problems that caused patients to get wrong drug doses and miss treatments. The problems: IVs ran longer than intended and information showed up on the wrong patient. If he finds the perfect information system anywhere in the world in all that investigating, I’d like to hear about it.
Frustrating: I bought those squiggly, energy-efficient Sylvania bulbs from Sam’s that say on the box they’ll last seven years. So far in one bathroom, four of six have burned out in just a handful of months. Ripoff?
John at Chilmark Research weighs in on the Medicity-Novo Innovations merger.
Simon Samaha MD, who we old timers remember as CIO of Cooper University Hospital, is named president and CEO of Summit Medical Group, a 140-physician medical practice in New Jersey.
McKinsey Quarterly noodles on Why Americans Pay more for Health Care. The big reason: outpatient care, which is theoretically cheaper than inpatient care, but only if it replaces it. One culprit CT and MRI scans, which makes it very profitable. Also: "Well-insured patients who bear little, if any, of the cost of their treatment have no incentive to be value-conscious health care consumers. Moreover, even if they wanted to be value conscious, they don’t know enough." Let’s repeat: providers will do whatever they can get paid to do, just like every other profession. It’s not illegal, immoral, or even harmful – it’s just expensive for whomever is picking up the tab (not the patient, in most cases). If you want them to stop, then don’t pay them for doing it.
As Inga mentions below, LinkedIn yanked my photo, a shot of the Unknown Comic. How do they know it wasn’t me wearing a bag? Here’s my thought: I’ll chose an HIStalk reader’s picture and put it on my profile. Then, I’ll see who recognizes them at HIMSS and ask them to report back whether they received any accolades, assaults, or indecent proposals. In fact, I could swap reader pictures once a month so that I am, in fact, an HIT Everyman or Everywoman.
MedAvant, rescued from bankruptcy in September by selling out to Marlin Equity, acquires the Medicare Crossover business of HDM.
The Motion Picture & Television Fund will close its hospital and nursing home in Woodland Hills, CA due to $10 million a year in operating losses, laying off 290 employees.
GE Healthcare announces the merging of its two Milwaukee area divisions, diagnostic systems in Waukesha and clinical systems in Wauwatosa (did they intentionally choose towns with odd yet similar names?) The company boldly claimed it was about growth, no doubt the same reason they’ve been laying employees off and closing plants. It’s also shutting down the GE Healthcare Lunar office in Madison, moving manufacturing to Milwaukee. Despite the oddball name, it makes equipment to measure bone mineral density.
In that vein and locale, Wheaton Franciscan also announces its latest growth strategy: the forced evacuation of another 100 or so employees on top of the 250 positions already eliminated. If you live in Waukesha County, watch out for traffic near the unemployment office.
<shameless self-aggrandizement>A New Zealand integrator working on an RFI there asked me a few weeks back if I would mention their interest in hearing from US software vendors who might participate in a big patient records project. I did and the company says they got more than a dozen inquiries. Also, from a company who ran a text ad like those you see to your right, "We have seen more clicks from your site than any other of our ad locations (Google, Yahoo, etc.). You have a great site and I love reading it every day." </shameless self-aggrandizement>
That’s an HTML joke above, in case you didn’t get it.

Planned business closings and layoffs, courtesy of CoStar Group: Irvine Regional Hospital and Medical Center (CA) was to close Thursday, laying off 510 employees (above). Health Research Association (CA), the clinical trial support organization of USC, will lay off 79 employees on January 30.
Odd lawsuit: the family of a man who died after elective spinal fusion surgery at specialty hospital West Texas Hospital is suing the now-closed facility, claiming its medical staff didn’t recognize his blocked airway complications. His wife repeatedly asked staff for help, the hospital PA covering the ED (!) was paged, nobody thought about establishing an airway, and the wife gave him CPR. The hospital’s action: they called 911.
Jonathan Bush is on CNBC again. He quotes the IOM report and rails against the government gravy train. Worth watching, even if the gaggle of amped up hosts constantly interrupts him at a nearly intolerable volume. "Pay for data, pay for results, and you can’t believe how fast doctors will get out there and get online."
Hospital layoffs: Gaylord Hospital (CT), 11; Wyoming Valley Health Care System (PA), 20; Banner Health (AZ), 334; Mt. Carmel Health System (OH), 300; Rogue Valley Medical Center (OR), 20.

The CEO of Carolinas HealthCare System is doing OK, though, having been paid $3.5 million in 2008. They claim he earned it, which at least is slightly different than the standard excuse of having to pay competitively to attract such notable talent to a non-profit endeavor.
E-mail me.
HERtalk by Inga
From LinkedIn Customer Service: “Re: your profile picture has been removed. The picture is in violation of the LinkedIn Photo Policy because it is not an accurate representation of you.” What? My avatar is absolutely an accurate representation of me (in an optimized, sexier, Barbie-ish sort of way.) Apparently only “photographs” are acceptable. Mr. H is also miffed because his profile picture (a photograph) was also removed. His was the one with the bag over his head, which apparently is one of Mrs. H’s favorites since he likes to wear the bag around the house all the time (I didn’t ask). I just posted a new photo of myself. We’ll see how long before that one is also removed.
I have to say the quality of the writing and commentary from our readers is amazing. In the last week we’ve had some excellent stuff out there, both on HIStalk and HIStalkPractice. Thanks to everyone taking the time to support our sites by providing thought-provoking, smart, and entertaining material. We are always looking for great content, so drop us a note if you have any HIT reflections to share.
Retired Gen. Eric Shinseki, Obama’s pick to head the VA, vows to develop an EHR for active duty personnel and veterans and make business practices as paper-less as possible. Shinseki tells senators during his confirmation hearing that the barriers have not been technical, but rooted in the VA and Defense department’s leadership.

Also on Capitol Hill, NQF CEO and President Janet Corrigan tells a Senate committee that effective use of HIT is essential to improve quality, safety, and affordability.
GE Healthcare confirms its former IDX Systems headquarters in Vermont is cutting staff and other costs. A GE spokesperson would not discuss the number of employees affected.
Hill-Rom Co. also confirms job cuts and operational consolidations. The company plans to cut about 450 positions in the US. Hill-Rom laid off 150 employees at the end of 2008.
If you’ve been affected by all the recent layoffs, perhaps it will make you feel mildly better to know that healthcare workers in other countries are also suffering. Swedish medical officials announces plans to cut 900 jobs (6% of the workforce) in order to reduce costs.
Toronto General Hospital pilots its first surgery checklist, aimed at reducing adverse events.

Here is a new must-have item for fashion-conscious, cold-fingered iPhone users. The thumb and index-fingers on these $40 gloves by North Face are covered with special fabric that includes silver.
Mr. H mentioned an odd lawsuit last week that involved a deaf patient who sued her doctor for failing to provide a sign language interpreter. She ended up winning $400,000. A company called LifeLinks saw the lawsuit as an opportunity to promote its remote translation services, which allow providers to connect with interpreters and sign language specialists via the Web. Providers only pay for the interpreters’ time, which undoubtedly costs far less than $400K.
Medicare beneficiaries in Arizona and Utah test new PHR software that includes two years worth of Medicare claims data. Patients can manually enter additional data. Some additional information can be uploaded electronically. Personally I think I would be more inclined to use an EHR that was pre-populated with at least some data, so this sounds like an interesting pilot.
University Hospitals (OH) launches a new physicians’ portal that combines electronic prescription writing with medication reconciliation.
Blue Shield of California Foundation announces its intent to stop issuing HIT grants, citing more pressing healthcare needs. Last year the foundation issued almost $11 million in HIT grants.
Two Illinois hospitals settle lawsuits alleging they overcharged uninsured patients tens of thousands of dollars. Resurrection Health Care and Advocate Health Care have agreed to recalculate bills and give refunds to needy patients eligible for free or discounted care. In addition, Resurrection will extend a 25% discount to all uninsured patients, regardless of income level.
Anne Arundel Medical Center (MD) implements VISion:Asset Management from Versus Technology to provide real-time tracking services for hospital assets.
Nuance Communications and IBM announce a licensing and technical services agreement to enhance and expand speech solutions, including incorporating IBM technology into Nuance’s speech products. Nuance will also purchase speech-related products from IBM. Nuance also reveals that Warburg Pincus has agreed to purchase $175 million of Nuance common stock. Nuance plans to spend some of the money on merger and acquisition activity. The purchase represents almost 17.4 million shares.
CSC wins a $265 million, 7.5-year contract to replace North Carolina’s Medicaid Management information system.
Polaris Venture Partners acquires a substantial interest in National Electronic Attachment, a provider of secure electronic data for claims attachments.
Telephone equipment maker Nortel Networks files for Chapter 11 bankruptcy protection

CareTech Solutions and EnovateIT team up to create a custom wall station for Crittenton Hospital Medical Center (MI). The e645 Computing Wall Station will be mounted into individual patient rooms for point of care documentation.
The University of Pennsylvania School of Nursing and Eclipsys form an academic partnership that will incorporate Eclipsys technology into the curriculum.
Tawam Hospital in Dubai goes live on Royal Philips’ iSite PACS, the first public hospital in the Middle East to do so. Tawam Hospital is affiliated with Johns Hopkins Medicine International.
E-mail Inga.
Pete Sanderson’s Responses to Comments from Yesterday’s Post
Comment #1
A partner and I are ramping up to start a consulting practice sharing best practices for HIT projects. We are consistently amazed at what a little project management rigor can do to keep the ship on course. Thanks, always interested to hear success stories and lessons learned on HIT projects.
Feel free to share a few of your success stories
Comment #2
I can understand that you don’t want people padding their budget estimates to ensure 100% success, but I also understand why someone might bristle at having their project labeled a failure for completing work too far ahead of schedule or producing something at a lower cost than expected. Much is learned during the course of a project, and it seems like you might inadvertently be disincentiving people from taking advantage of optimization opportunities.
Good point. Every project includes identifying named human resources to accomplish tasks and achieve deliverables. You identify named resources to make sure they are not over allocated. You seek to avoid asking someone to do 100 hours worth of tasks during a 40-hour work week. As you learn during the course of the project, you produce change requests that either free up resources or seek additional resources for your project. The Project Management Office balances all the change requests from a portfolio of projects trying to balance organizational priorities and resource availability. It can be tricky, but allows the organization to track projects and provide adequate resources where and when needed. An added benefit is the ability to forecast needs and being proactive to meet needs months down the road.
Comment #4
‘Good process and leadership trumps bad software.’ There are some many things wrong with this statement I don’t know where to start. Suffice it to say I completely disagree. Nothing trumps bad software.
With truly bad software, you are correct. The statement should really read, "Good process and leadership trumps marginal software or software that is mislabeled as bad software." How many times have you replaced a product thought of as bad software only to find the problem has not been fixed? We often find our trouble with software is due more to how we have chosen to implement it rather than with the software itself. The point is, business leaders should optimize processes and use of the software before deciding the software is truly bad. Good process and leadership can often improve the use of software mislabeled as bad saving the time and cost of implementing a new product.
E-mail Pete.











































RE the AI GLP1 company, Washington Post has an article today by someone who used one of those compounded products,…