

Giving a patient medications in the ER, having them pop positive on a test, and then withholding further medications because…
Monday Morning Update 1/12/09
From You Missed This: "Re: another e-mail blunder from an HIT CEO." Eclipsys CEO Andy Eckert accidentally copies an equities analyst from Thomas Weisel Partners on what was supposed to be a private e-mail to CFO Bob Colletti and EVP Jay Deady, in which he remarked that a Weisel research note questioning the company’s growth rates, "certainly zeroed in on our organic growth rate." Andy told the analyst that what he was saying is that organic growth is a focus, not admitting that Weisel had uncovered a weakness. Still, the analyst’s generally positive opinion didn’t change.
From oneHITwonder: "Re: Sutter. My father was recently a patient at Sutter General Hospital in Sacramento (he’s home and doing well now). While visiting, I watched a nurse enter his room and pull down a wall-type desk, which revealed a keyboard and monitor. I was very impressed, but the nurse did not use the computer — she just pushed the keyboard out of the way and used the desk for a writing surface. I later asked another nurse if she uses the computer in the room and she said only if all the workstations at the nurses’ station are being used. Another nurse joined in, saying they were put in the room for ‘e-charting’ that never materialized, assuming ‘it must not be going well at other Sutter hospitals’ (I believe the reference here was to Epic). They occasionally look up lab orders, but that is about it. Sutter General uses Eclipsys for CPOE."

From The PACS Designer: "Re: Palm phone. Palm has released its challenge to the iPhone and it created quite a stir at the Consumer Electronics Show. Perhaps there’s a place in healthcare for the new Palm Pre to support user requests to add it to existing systems." Link.
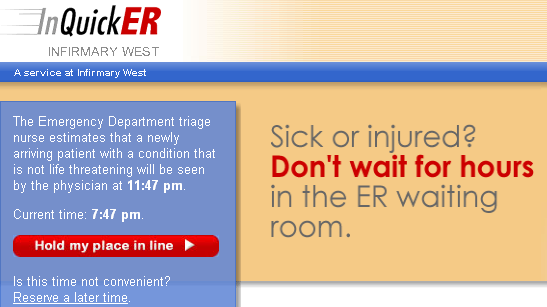
This sounds interesting: Infirmary West (AL) launches an Internet system that lets patients self-register (for a $25 fee) for non-life threatening ED appointments, then come in at the appointed time instead of sitting around watching Judge Judy amidst the mayhem. They take it seriously: if the patient isn’t seen within 15 minutes of their appointed time, their visit is free. The nurse who runs the ED came up with the idea. An employee checks each registration as it comes in to make sure the patient’s condition doesn’t require immediate evaluation. Notice that the registration screen also provides an estimate of when you’ll be seen even before you sign up. The system provider is InQuickER, which runs the same service for several hospitals, but I can’t find out anything about the company.
A reader sent over a local article about December layoffs at North Memorial and Park Nicollet in Minnesota that were to affect over 600 positions.
Medfusion, the Raleigh, NC vendor of consumer-facing technologies for physician practices (like patient messaging, online registration, online payments, etc.) buys the former A4 and Allscripts office building in nearby Cary for $7.25 million, citing strong sales and the need to add up to 50 employees to join the current 70 in 2009.
Tennessee RHIO Shared Health hires Adnane Khalil, formerly of MedAvant, as VP of technology.
I’m doing some tentative experimentation with Twitter, so if you want to follow me, I’ve put an icon over in the right column. You won’t get much except updates when I publish something new, at least until I make it part of my routine. I might use it from HIMSS.
The CFO of Misys PLC resigns "by mutual consent."
Last chance for HISsies nominations. When the voting starts, you’ll say, "Why didn’t that idiot include these obvious nominees?" and I will smugly respond, "Because you and your passive ilk couldn’t be bothered to click a simple link to nominate them." To avoid all that unpleasantness between us, you might as well cast your nominations.
Nobody likes it when welfare recipients complain about the free money they get from the rest of us, so maybe HIMSS should be careful about how it characterizes its EMR Welfare Program. In Modern Healthcare, its director of congressional affairs is quoted as saying, "Our minimum is $25 billion."
I’ve never heard of Leap of Faith Technologies of Crystal Lake, IL, but the eHealth technology vendor is looking for testers for its "virtual pillbox" for smart phones. The eMedmobile application extracts information "smart labels" on pharmacy containers to issue medication reminders and to notify someone if the patient misses doses. Grants to help cover its development cost came from NIH, the National Cancer Institute, and the National Institute on Aging. Check out the demo – it’s cooler than it sounds.

Interesting: medical students at University of Washington practice surgical technique in a mocked-up OR that includes a computerized patient. What’s different is that they’re also using simulations like these for nurses, dentists, and pharmacists and will combine the programs to teach the professionals communicate better, not just to practice their technique. A good line from the executive director of UW’s Institute for Simulation and Interprofessional Studies on the traditional surgeon’s training of learning on live patients: "I’d rather be able to tell some surgical resident, after 25 unsuccessful tries on a simulated patient, that maybe he ought to consider going into pathology.” UW is is also trying to get Microsoft to adapt the Xbox to allow training students at remote locations, but apparently hasn’t had much luck.
Reports suggest that troubled Satyam Computer Services is looking for a buyer. The CEO was arrested and the board dissolved this week after admitting that revenue was overstated and $1 billion of cash assets did not exist. Law firms are lining up to get a shot at the lawsuit coming against auditors PricewaterhouseCoopers, about which one big equity firm’s head said, "If you’re an auditing company and your client says they have $1 billion in cash, you do check with the bank." The company’s interim CEO was formerly president of its commercial and healthcare businesses.
Cardinal Health cuts its fiscal year outlook, citing hospital cutbacks in capital spending.
I’m guessing Bush and Obama don’t agree on much (thank goodness), but here’s one goal both think is important: having electronic health records for all Americans by 2014 (and that you can deficit-spend your way out of a depression, apparently). In a speech Thursday, Obama said the government will make "immediate investments" on IT, which will not only save money, but "reduce the deadly but preventable medical errors that pervade our health-care system." With that in mind, Gerson Lehrman Group predicts a 14.1% annual growth in the EMR market, although they oddly list Google and Microsoft as big potential winners (and also GE and Siemens, whose products I sure wouldn’t want my taxpayer dollars to fund if it’s innovation that’s needed). It’s funny that the Republican pushed free open source solutions like VistA, while the Democrat seems to be in favor of just buying commercial products with federal money. You’d think it would be the other way around, although not when the goal is just to spend a bunch of government money.
With that in mind, new poll to your right: where should the billions be spent?
Hospital layoffs: Good Samaritan (NE), 32; St. Francis (NE), 22; Blue Hill Memorial Hospital (ME), no number given; University of Chicago Medical Center (IL), up to 1,000; St. John’s Regional Medical Center (CA), 33; Los Robles Hospital & Medical Center (CA), 8; Ventura County Medical Center (CA), 30; Central Kansas Medical Center (KS), 50; Carson Tahoe Regional Healthcare (NV), 30; Erlanger Medical Center (TN), 80. Tenet Healthcare announces cuts in vacation time, sick time, and 401k contributions for its 50,000 employees. CGH Medical Center (IL) shuts down its free nurse hotline that gets over 550 calls a week.
West Penn Hospital says it fixed a patient-reported problem in which its online bill payment application that allowed users to see information about other patients. The hospital blamed a billing partner, but didn’t explain why the patient e-mailed the hospital twice and didn’t get a response until she called the local TV station.
More on the National Research Council’s Report on Healthcare IT
I worked late Friday night to get a summary of the report out because I think it’s important. I’m already getting some thoughts back from folks in the industry, so I think we’ll have a good dialog about what it means.
Much of what I’ve written in the past aligns with what the report says. In 2005, I cited an excellent report from The Advisory Board Company as the basis for an editorial on the shortcomings of clinical systems like CPOE, which the report said fails to improve practitioner performance 87% of the time. I said, "Several years after the IOM report that supposedly opened our eyes, clinical systems really haven’t delivered on the expectations. They haven’t made us much better … Everyone is buying and implementing and improving, but the patient doesn’t seem to get much benefit from all this clinical system churning. We’re still plagued with poor integration, sloppily designed bolt-ons to old products, and outdated architecture. We’re also not good at changing business processes on the provider side, so let’s take a few lumps along with our vendors. We’re equally guilty."
The logical question people might ask themselves: I agree with the report to some extent, so what happens next? Will the conclusions cause years of sustained activity and industry self-reflection like IOM’s "To Err is Human"? Some thoughts:
- Who’s going to pay for all this clinical and IT improvement?
- Is the IOM’s vision of patient care a reality or a pipe dream? Will hospitals commit to it? If not, there’s no reason to build automation that won’t be used – we already have that problem.
- Show the numbers that justify the cost. Did UPMC’s cost or outcomes improve after they spent tons on IT? Are they better than less-automated facilities? So far, the link between IT investment and excellence (of any kind) seems iffy, especially when held to the standard that IT caused the improvement, not just co-existed with it.
- The report suggests that a complete shift in systems development, implementation, and use is needed. So how do you put that into play, especially in a competitive IT market where vendors can’t just scrap what they have and start over? And in a competitive provider market that’s struggling with low margins and entrenched inefficiency?
- Were conservative CIOs part of the problem, happy to ditch best-of-breed systems in order to gain integrated mediocrity that’s easier to support? And is that still necessary with more modern integration technologies? All of those systems were designed even before the Internet caught on.
- Maybe the next step would be to create specific standards from those goals that could be used to assess specific systems and their use. I’ve often said that a big problem with clinical systems is "having them" vs. "using them to improve care."
- The challenge will be the lack of standards in hospitals, even the lack of repeatable processes within a given hospital. Hospitals are notoriously unwilling or unable to get employees and physicians to follow even obviously important rules (like "wash your hands"). Systems are hard to support and enhance because hospitals resist change, forcing vendors to build in an infinite number of configuration options.
- The committee intends to follow this report with others, although in the case of "To Err is Human," most of the reaction came from the shock and public shame of the first one (Googling "98,000 medical errors" gives 83,000 hits).
- It will be interesting to see how HIMSS reacts. My first thought was that it would rush out a vindictive, clearly vendor-serving defense like it did with Ross Koppel’s articles, where he studied the unintended consequences of a clinical system implementation that actually increased patient harm, and HIMSS took offense. I think they’re smarter now, though, and will simply suggest more research while staying the course, i.e. still insist that the government should subsidize the purchase of today’s EMR systems, which is diametrically opposite to what the report concludes. HIMSS sees itself as the voice of healthcare IT, so it will surely recommend actions in which it (and organizations it influences) will be a prominent player.
- With that in mind, the last organization that I would want at the table when discussing healthcare IT changes is HIMSS. No offense to them, but their world is high-paying vendor members and flashy exhibit halls, not upsetting the gravy train. The approaches IOM says are wrong are the ones HIMSS pushed us into: RHIOs, CPOE, and "clinical transformation" that rarely had any impact.
- Nothing in the report should be interpreted as blaming vendors for anything. It merely says, "We’re here and we need to change direction to go to there." The job of vendors is to sell what customers will buy, so I take the conclusions as more of a criticism of providers who not only don’t demand systems that might work differently, they don’t even use the ones they have optimally. Providers should be setting the vision, not vendors, but have shown a remarkable inability to do so. Still, current products were based on old paradigms and old technologies, so it’s a good time for vendors to take stock.
- Despite the long list of problems in the report, it should be noticed that some hospitals have had success (quiet or otherwise) using off-the-shelf systems. I see it like this: today’s systems have taken us about as far as they can, hopefully providing value and benefit along with way. Now we’re ready to envision the second generation of systems (I’m arguing that we’re still in the first generation, but you may disagree), assuming that providers are simultaneously ready to embrace the changes that these new systems will support.
- Software vendors and hospitals dedicate a huge chunk of resources to billing and malpractice avoidance. If you want to reform healthcare and healthcare IT, simplify payment and free up all those people working on billing and other administrivia to do something that actually benefits patients.
- If you want to know what a given person or organization will excel at, look at what they’re paid to do. If you want someone to change their behaviors, make sure you’re rewarding the behaviors you want. If you’re paying someone to paint your house, don’t base their pay on what they spend for paint.
- The bottom line: the goal is measurable quality improvement and reduced cost, not conspicuous consumption of IT. If you pay people to deliver better and cheaper outcomes, they’ll figure out what tools they need.
It is time for the Jedi Knight to revolt and take back the practice of medicine from the Dark Side. Does Doctor of Medicine really stand for Doctor of Healthcare practice? If MDs did not have to admit, would there be such enormous economic obesity in healthcare? Don’t really know where I want to go with this but practicing medicine with a license is the high paying profession in a box to be exploited by the process we all know as healthcare.
The healthcare people take this “box” and sell it like a commercial product just like Macy’s. Sure the medical staffs in our hospitals have a voice but is it really a collective voice that is acted upon or just politics as usual? Maybe, just maybe if just a few MDs would band together without attending patient responsibilities and tell the world what they need to avoid medical misadventure (medical error, it is not called healthcare error) then perhaps assemble a club of medicine men called Medical Information Systems Society Systems (MISSM). Sham-Wow it sounds like the IOM.
Correction: Medical Information Management Systems Society (MIMSS). You following me IT Guy?
The Sutter thing is a blown Eclipsys install. They failed on the eCharting. Epic is replacing that initiative, but it take Sutter a long time to get through things.
One of the most telling tidbits I gleaned from the IOM report I gathered was the fact that we have been automating the “business” of medicine for a long time and not the “practice” of medicine. Although the many desperate system “collect” a lot of healthcare data, few gather it into an actionable set of information which is available to clinicians at the point of care to enable “cognition” (also emphasized in the report). Putting the already collected data into a resource for doctors to see and be able to make better informed decisions about the care they are giving seems to be the key. Once that occurs, doctors (the scientist they are) will begin to act differently and improve the quality, efficiency and the efficacy of what they do naturally.
Has anyone heard about the terrible financial epic project at Cedars Sinai in LA? They have not done good testing (do not even have a singel test plan to include interfaces and conversion data) but still are planning on deployment on 3/1! The team is being run buy the same resources who ran the last deployment of PCX which caused a revolt and made the nationwide news. Too bad of the celebs who give them endowments do not know how their money is being wasted!
From the IOM posting –
This is an interesting group: mostly computer experts who could bring an objective viewpoint to the table (no vendors, no advocacy people, no caregivers).
No bias? No motives? No for profit interests?
Who checked these guys out ahead of time? Does Intel tip it’s hand below? Does Google or MS have any “monetization” interest in healthcare search?
And, what group of professors in a room with Google and Intel won’t be thinking about funding sources for their next projects.
This report wasn’t at all balanced. Sad.
The Intel® SOA Expressway for Healthcare (Intel® SOAE-H) provides a highly efficient way to get computable healthcare information from one place to another—across departmental systems, among providers, and to a regional or national group supporting a healthcare community. Moreover, its vendor-neutral platform makes it suitable for inclusion in healthcare vendors’ product offerings, allowing vendors of all types to modernize and expand their markets within or across the healthcare environment. This enables healthcare providers to develop integrated digital hospitals that improve quality of care, workflow, costs, and accessibility.
Product overview
A key reason for the slow adoption of sharing patient information in healthcare environments is the high and variable cost of proprietary data and integration services. The Intel SOAE-H uniquely offers cost-containment and operational simplicity by providing a high-performance platform-based solution for translating, processing, and connecting multiple data formats across a healthcare environment.
The Intel SOAE-H combines robust HL7, EDI, and HIPAA support and a unique healthcare environment developer kit (HDK) with a high-performance, codeless workflow engine, native XML acceleration, and appliance manageability in a simple software form factor.
It can be used in a stand-alone manner to construct large multi-site health networks using the HDK, or it can be used as a base platform to augment healthcare vendor product offerings with a modern, high-performance SOA-based architecture. In either case, the goal is the same—to accelerate computable healthcare information across disparate health environments such as hospitals, integrated delivery networks, clinics, payor networks, labs, and pharmaceutical networks.
Unmatched time-to-value realization
By using the Intel SOAE-H, many common integration problems can be addressed entirely within a visual environment. Extensibility features ensure that complex integration is easily addressed. Further compression of time-to-value comes from familiar BPEL design-time environment and SOA manageability tooling.
Rapid implementation
The Intel SOAE-H can be up and running in as little as 60 days or less—even in complex network and data center environments. Its “codeless” design means that organizations can leverage built-in services, and design tools to map and manage outgoing and inbound content without the assistance of expensive and scarce software development resources, and can connect to networks through multiple, open standards-based communications protocols. The WS-BPEL-based workflow design makes development as simple as “configure-deploy-run,” and reduces coding of standard data flows.
Agreeing with Sutter Intel. I believe they have Epic up at several ambulatory sites. Only now are they in the process of implementing Epic in an acute setting and that’s out in their Western Region. It probably will be a while before you’ll see Epic in Cow-town.
A stand alone prepublication PDF of the report is at this link at NLM: http://www.nlm.nih.gov/pubs/reports/comptech_prepub.pdf
You’re right, not many in industry will like this report, but neither was the Flexner Report on medical education and certification liked when it appeared a century ago.
However, to not act on this report and the Dec. 2008 Joint Commission Sentinel Event Alert, and to continue with the status quo is unacceptable. I predict that not acting will result in painful marketplace failures and litigation. Not to mention adding a new angle to malpractice litigation.
The findings are hopefully going to be beneficial towards the improvement of healthcare.
I think the informatics and medical communities owe a debt of gratitude to the editors and contributors who made this report possible. It is a bit daring in some ways.
The report addresses HIT’s issues in a sober, scientific manner. It is a contretemps to the irrationalism, neglect of scientific principles and colorful marketing that seems to have developed in the industry in recent years that’s led to corporate claims that HIT will ipso facto “revolutionize healthcare” as well as paradoxical HIT leadership structures.
I would welcome a return to sound scientific approaches to HIT design, deployment and diffusion, with a purpose of facilitating healthcare and HC professionals (not “revolutionizing” it, whatever that means), to replace a marketing and profit driven exuberance that seems a characteristic of HIT, and perhaps all IT, today.
I hope this report and the recent Joint Commission Sentinel Event Alert on HIT will foster a return in HIT to the scientific rigor of medicine itself.
It does tend to validate the work of a relatively small group of us in Biomedical Informatics, IT-Sociology, and related fields. In my case I’ve been writing on these issues for over ten years, after observations as a CMIO at a large hospital.
Dr. Octo Barnett at Harvard, one of the contributors and an informatics pioneer, goes back further. The report could be considered a fleshing out of his “Ten Commandments” for HIT, addressing why healthcare was not receiving the benefits expected of HIT.
Dr. Barnett wrote his “Ten Commandments” in 1970. Others wrote on similar issues back then as well.
These can be seen in “A History of Medical Informatics in the United States 1950-1990″ (pp. 167-175), Morris F. Collen B.E.E., M.D., 1995, American Medical Informatics Association, ISBN 0-9647743-0-5.
Scot Silverstein
Drexel University
Institute for Healthcare Informatics
Philadelphia, PA
Mr. Obvious writes:
“This report wasn’t at all balanced. Sad.”
Actually, the report was backed up by empirical evidence, unlike your statement that it “wasn’t balanced.”