

News 7/21/17
Top News

Athenahealth reports Q2 results: revenue up 15 percent, adjusted EPS $0.51 vs. $0.34, beating expectations for both.
ATHN shares rose 7 percent in after-hours trading following the announcement. They’re up 15 percent in the past one year and 54 percent in the past five, but both significantly trail the performance of the Nasdaq index.
The company’s market value is $5.7 billion. Co-founder, CEO, and board chair Jonathan Bush holds shares worth about $45 million.
Activist investor Elliot Management disclosed in May 2017 that it had acquired 9.2 percent of the company’s outstanding shares and will try to force the company to consider “strategic opportunities.”
Reader Comments


From e(x)HMP: “Re: David Waltman’s golden parachute at Cerner. Not the first time he has found a way to fail upwards. He represents everything that is wrong with the VA/VistA fiasco. By all means, let’s give this guy a third shot.” The reader linked to a 2013 story about the VA’s $162.5 million contract award to ASM Research to improve the user experience with VistA, triple the price offered by two competitive bidders. One month later, the VA’s David Waltman – who had worked on the contract as chief UX architect of the iEHR project – announced that he would be leaving to take a chief strategy officer job with Accenture-owned ASM. ASM’s subcontractor in the project was Agilex, which had hired former VA CIO Roger Baker. Waltman lasted only nine months at ASM before going back to the VA as chief information strategy officer. Baker worked two years for Agilex, which was then also acquired by Accenture.

From Soft Machine: “Re: Teladoc and Analyte Health. Definitely headed toward covalent bonding. What do you make of them?” Analyte Health offers telehealth providers lab ordering, specimen collection, and testing services. The CEO is industry long-timer Kevin Weinstein, who was chief growth officer at Valence Health through its acquisition by Evolent Health. Teladoc and Analyte health announced a partnership in January 2017. Being a hospital guy, I’m not crazy about Teladoc’s model since I can’t fathom why hospitals don’t launch their own branded telehealth service with their own doctors and keep patients within their system (no different than retail clinics), but TDOC shares have doubled in price in the past year to a $2 billion market cap, giving the company money to use for acquisitions. Analyte Health would be a significant differentiator since many telehealth encounters involve an awkward lab test handoff and having integrated lab services opens the door to offering services for conditions beyond the usual rashes and ear infections. Hospitals that compete with or are indifferent to Teladoc might like working with Analyte Health since it doesn’t run its own labs – it contracts with hospitals and commercial lab providers and thus could steer business to the hospital lab.
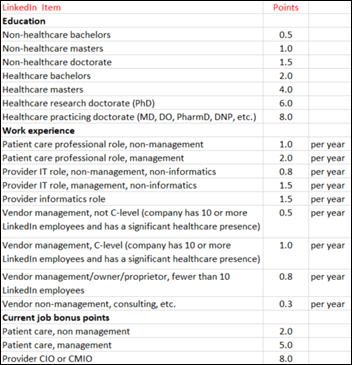
From Aging Programmer: “Re: your HIT index. Loved it! I scored myself and got an 82. The main potential issue I see is the definition of management – maybe it should be managing at least five employees, in which case my score drops to 67. Ironically, my consulting time had almost as much impact as my CMIO experience, but I know there’s a lot of dead wood consultants out there.” I reviewed AP’s LinkedIn and I think his very high score of 82 seems about right given his medical education and extensive provider experience that emphasized informatics. I thought about trying to define the scope of management, but the only person who would know that is the individual since LinkedIn only lists titles, so I think you get points for title regardless of actual responsibility. In comparison, quite a few of the “most influential” folks would score in the low single digits with no healthcare-related education or significant health/health IT work experience. I’m certain many of them would protest that their speaking engagements, unpaid advisory board participation, and blog posts should boost their scores, but I don’t see how those necessarily qualify someone to render analysis and opinion. Nobody pays much attention to what armchair quarterbacks and barstool coaches think about football.
From Scribe Feedback: “Re: scribes. I’ve had two experiences with scribes in the past two weeks. The PCP scribe was new and could not navigate Epic well. The PCP was also coaching someone, so I was outnumbered four to one by the PCP, scribe, MD-to-be, and the nurse. The PCP spent 80 percent of his time focusing on the scribe and the person he was coaching while communicating with the nurse. The second interaction with the specialist was very good – he kept his eyes on me and after explaining the role of the scribe, it was like she wasn’t even in the room. The specialist also uses Epic. I’m not sure if the PCP’s documentation requirements caused the difference, but there has got to be a way to make the scribe less intrusive.”
From Can Spam: “Re: Athenahealth turnover. The amount of churn is remarkable. Since 2015, they’ve lost their chief technology and product officer, COO, two CFOs, and the VP who was instrumental in building AthenaNet. Likely more to come given the involvement of activist investor Elliott Management.” Investors have reacted positively to Elliott’s involvement (as they often do), although customers should probably be less enthused since it’s not necessarily in their best interest to have the company sold or broken up into more lucrative pieces.
HIStalk Announcements and Requests

We’ll be missing Dr. Jayne’s regularly scheduled post tonight as she struggles (yet again) with the Microsoft Surface she unwisely purchased that seems to have given her constant problems since. This time a software update killed it.
This week on HIStalk Practice: Waud Capital Partners acquires ChiroTouch. Nebraska HHS, HIE work with DrFirst to advance PDMP. Cow Creek Health & Wellness Center rips and replaces with help from Greenway. Solo family physicians advocate for low-cost, easy-to-use patient-generated data tools. New CDC director takesTwitter for a spin. Carolina Center for Occupational Health goes with Bizmatics HIT. Tom Lee, MD hands over One Medical reigns. North Carolina health officials find themselves in hot water due to a trail of data entry oversights.
Webinars
None scheduled soon. Previous webinars are on our YouTube channel. Contact Lorre for information on webinar services.
Acquisitions, Funding, Business, and Stock

Netsmart acquires home care and hospice software vendor DeVero.

The State of New York provides $2 million in tax breaks to electronic referrals vendor EHealth Technologies, which will expand its 215-employee Henrietta operations in adding 160 full-time positions in the Finger Lakes area.

EHR security tools vendor Protenus raises $3 million in an extension of its Series A funding round that has raised $7 million.

Private equity firm Waud Capital Partners acquires chiropractic software vendor ChiroTouch from private equity firm K1 Capital, installing its own CEO as part of the “partnership.”

In the United Arab Emirates, Emirates Hospital — owned by UAE-based investment group KBBO – buys a 60 percent position in Dubai-headquartered MD 24-7, which offers online and face-to-face wellness and concierge services.
Sales
Medical Associates of Clinton, IA chooses EClinicalWorks 10e cloud-based EHR for its 49 providers.
People


PokitDok hires Joe Murad (Willis Towers Watson) as CEO and board member. He replaces co-founder Lisa Maki, who remains on the company’s board.

AHIMA announces in a member email that CEO Lynne Thomas Gordon’s last day was July 15, although it did not provide a reason for her departure. A search for her replacement is underway.


Home care software vendor HHAeXchange promotes Greg Strobel to president and CEO. Founder and former CEO Raphael Nadel will become chief innovation and strategy officer.

Missy Krasner (Box) reportedly joins Amazon in unannounced healthcare role.
Announcements and Implementations

Arizona Pulmonary Specialists (AZ) and Harbor-UCLA Medical Center (CA) go live on ZappRx’s specialty medication drug prescribing platform, with the director of Harbor-UCLA’s pulmonary hypertension center saying its first prescription was approved within 48 hours vs. the common paper-based process that sometimes took more than three weeks.

Three of North Carolina’s largest health systems – Novant Health, Carolinas HealthCare System, and Duke Health – will connect to the state-operated HIE NC HealthConnex, which also announced that the Coastal Connect regional HIE will join.

Seventy-bed Jones Memorial Hospital (NY) and two other hospitals affiliated with UR Medicine receive a $5.7 million state healthcare transformation grant to replace Meditech and LSS with UR’s Epic system.

In Ireland, a former hospital CEO develops CliniShift, a staffing app that allows a hospital to match its vacant shifts with available staff. It also tracks the status of credentials and allows managers to monitor how the app is being used. The company expects to begin a pilot project at an unnamed large hospital on the US East Coast in September and has opened an office in Boston.
Meditech announces that it will offer CommonWell interoperability services in early 2018.
Change Healthcare joins the Hashed Health blockchain technology consortium.
Government and Politics

England’s NHS Digital responds to a review of its practices that notes ambiguous expectations, a lack of centralization of innovative ideas, worse than expected feedback fro its data services customers, and reliance on outdated technologies. NHS Digital says it will:
- Implement an effective enterprise architecture function
- Create a service operations capability and future roadmap
- Standardize delivery methodologies
- Create a build vs. buy strategy
- Develop a unified security model and security operations center
- Implement new business intelligence and customer relationship management tools
- Work more closely with stakeholders
- Create a thought leadership program
- Create an investment approval subcommittee of the NHS Digital Board
- Set up a workforce planning center to extend recruitment and review the eight office locations
An investigative article finds that HHS is using taxpayer money that was intended to promote Affordable Care Act insurance signups to instead fund a PR campaign against it, creating videos of people who claim to have been harmed by the ACA. The White House chose the video subjects and flew them to Washington DC, with some of those participants later saying that the HHS people pushed them into being more negative about the ACA than they really feel. Former CMS Acting Administrator Andy Slavitt commented, “Congress appropriates funds for you to carry out laws they passed, not to spend those funds on activities that counteract those laws.”
Privacy and Security
Japan will take “strict action” against drug maker Bayer, which acknowledges that three of its employees inappropriately accessed survey-generated patient data to plan a promotion for the company’s Xarelto blood thinner.
Fortified Health Security releases its mid-year cybersecurity report.
Other


Sherpaa founder Jay Parkinson, MD, MPH blasts the venture capitalists who funded his company, then tried to liquidate it given the inherent disconnect between the VC desire to quickly scale and sell out vs. the “glacially-moving industry” of healthcare. Sherpaa’s handful of employed doctors offer online-only routine primary care encounters, charging individual customers $270 per year for unlimited app visits 24×7, which includes managing prescriptions, lab tests, referrals, and second opinions. Parkinson said the investor made himself CEO and then fired all the staff, including the doctors who could not legally stop seeing patients without giving them advance notice. He also accuses the investor of sending the company’s primary competitor, One Medical, its client and payments list in unsuccessfully trying to sell the company. The investor/CEO and board finally resigned a year ago and left the company’s remains for Parkinson to revive, but Parkinson says One Medical’s sales team then used Sherpaa’s proprietary information to badmouth it and to undercut Sherpaa’s employer rates. It’s an interesting idea and certainly cost-effective given the expense and overhead of arranging a PCP visit, but I would have to wonder how the VC was pitched in the first place. The company requires no upfront fee or ongoing commitment, so anyone who wants to give it a shot only has to pay the the first month’s $25 and then request a visit. I’m not sure how their doctors handle prescribing across state lines or how they manage referrals that are within the customer’s insurance network.

An insightful editorial says it’s counterproductive to call someone who is experiencing g a horrible disease – specifically Sen. John McCain – a “fighter” since the “warrior rhetoric” doesn’t improve their outcomes and can cause them to feel that they’re letting people down if they struggle or if they wisely choose palliative care instead of suffering through more rounds of painful treatments that offer little chance of success.

A Cancun, Mexico hospitals refuses to allow a premature baby to be transported back home to the US until the parents pay $30,000. That solved Mexico problem preceded the inevitable US one – the grandparents paid $18,000 for air transport to a Florida hospital that refused to accept the baby because of the mother’s Indiana Medicaid insurance, so now they’ll have to pay another $30,000 to get him to Indiana.
Sponsor Updates
- Liaison Technologies awards its first data-inspired Future Scholarship to high school graduate Antonio Ferris of Mesa, AZ.
- Tech.MN includes LogicStream Health in “The Ultimate Guide To HealthTech in Minnesota.”
- Santa Rosa Consulting is named a “best place to work”by Modern Healthcare for the sixth consecutive year .
- Optimum Healthcare IT is named one of the 50 fastest-growing companies in Northeast Florida for the second straight year.
- LogicWorks partners with CloudHealth Technologies to optimize cloud management and performance.
- Meditech will exhibit at the AHA 2017 Leadership Summit July 27-29 in San Diego.
- Obix Perinatal Data System, developed by Clinical Computer Systems, will exhibit at the AWHONN Florida Section Conference July 27-28 in Ponte Vedra, FL.
- Experian Health receives the 2017 MongoDB Innovation Award in the healthcare category.
- PatientSafe Solutions joins the Integrating the HealthCare Enterprise as a member organization.
Blog Posts
- The Hidden Costs of Dirty Orders (Liaison Technologies)
- Centralized Appointment Scheduling Aids Patient Experience (MedData)
- How to utilize CPT 99490 to increase revenue opportunities (Meditech)
- In a Troubled Healthcare System, ‘Digital Empathy’ is the Way Forward (HealthLoop)
- The CY2018 Medicare Physician Fee Schedule Proposed Rule – The Upshot (National Decision Support Co.)
- A Day in the Life: You Know You’re a Practice Administrator When … (Navicure)
- Clinical Alerting: The Key to a More Intelligently Connected Hospital (Spok)
- Passion and Vision for the Future: The Legacy of Neal Patterson (Netsmart)
- The Friction at the Gala: Getting to know the “Solver in Chief” (NTT Data Services)
- Helping Hands, CloudWave and Community Hospitals (CloudWave)
- Why Chronic Conditions Need Continuous Care Coordination (PatientPing)
- The Real Health IT Prize (PatientKeeper)
Contacts
Mr. H, Lorre, Jenn, Dr. Jayne, Lt. Dan.
More news: HIStalk Practice, HIStalk Connect.
Get HIStalk updates. Send news or rumors.
Contact us.














 e
e








































































RE the AI GLP1 company, Washington Post has an article today by someone who used one of those compounded products,…