

Thomas told me when he submitted his article that it was OK if I didn't run it because people generally…
News 12/5/08
From Cheryl: "Re: low-cost IT projects. I have been starving to hear stories like these! Leonard and Larry shared common problems, not hospital-specific issues. I am always on the lookout for how others are doing things better, especially solutions that can become best practices. To discover how these guys solved solved problems with easy-to-implement, cost effective solutions makes my little heart sing. Thanks for a truly valuable read! I want more! Cheers to Leonard and Larry. My new BFFs." If you, too, want to be Cheryl’s BFF (and who doesn’t?) then e-mail me your own small-project success stories. We may focus on big-ticket, multi-year endeavors most of the time, but somebody’s job could be saved by executing a quick and dirty project whose idea came from here, so give it up.
From Barney Chavous: "Re: BlackBerry improvement project. Can you provide contact information for Leonard Kravitz?" Ordinarily, no — I always provide a fake name unless someone asks specifically that I run their real name. In this case, Leonard (Lenny Kravitz, get it?) says it’s OK since a couple of folks asked: he’s Chris O’Connor, MD, FRCPC, Director of Medical Informatics, Trillium Health Centre, Mississauga, Ontario. He’s also involved with Open Source Order Sets, a project to roll out evidence-based content in Canada shared among contributors (great idea). You can e-mail him there. I found a BlackBerry writeup about the project he mentioned, which included his picture above. They did a Q&A and I liked this from him (it’s from 2006): "It is now remarkable to me, that in 2006, people are still using receive-only numeric pagers. It is the worst possible communication tool one can use, and yet it is the norm in medicine today. I still remember Pager Liberation Day: the day I released my pager and it sailed down to the bottom of the garbage pail and I never saw it again. That was fantastic and I have never looked back."
From OK in UK: "Re: iSoft. Any idea what happened to Paul Richards?" Link. Richards is replaced as iSoft’s managing director of the UK and Ireland by Adrian Stevens of Agfa. I don’t know where he went.
From Jade East: "Re: e-prescribing bonus. How did you guys come up with a maximum incentive of $1,600 per year? I cannot find anything that shows a capped amount." We actually said "average," not "maximum." That number has been reported in several articles, including the one we referenced that quoted a CMS administrator directly.
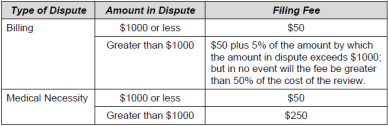
From Katrina Waves: "Re: insurance requiring that providers pay for claims appeals. Do you know of any documentation to substantiate this?" The reader did not provide a link, but being an intrepid Internet sleuth, I came up with this BCBS of NC document (warning: PDF – relevant part above). Want to know why they’re doing it? Because they can.
From H.I. McDonough: "Re: newsletter editorial. That was a great column. I wonder if anybody got it?" I wrote a particularly manic guest editorial this week for Inside Healthcare Computing called Camping Out for a Cerner Black Friday Door-Buster Special: Mr. HIStalk’s Plan to Stimulate the HIT Economy By Encouraging Unrestrained Holiday Season Greed, in which I advocated an HIT Black Friday sale (with major sarcasm). Above is an amuse-bouche clearly illlustrating my run-on sentence enthusiasm. Eat my literary dust, Pliny the Elder.
I have to learn to quit shooting off my mouth now that I have more readers. A nice person from Vanderbilt (you will be meeting him soon in "An HIT Moment with …") apologized that their article about moving from an HIT-rich environment to the technological boondocks seemed smug (my word). A good point: the article actually argued that the high-tech hospital has the responsibility to teach its trainees to work with more common low-tech systems like paper charts. I asked him to be our guest in a mini-interview and he’s up for it, so stay tuned. That’s pretty cool, especially instead of apologizing (a sly move!) he could have ripped me a new one for my cheekiness, although if he reads here, he’s probably used to that.
I ran a rumor of a possible ONCHIT candidate, so now you get a chance to influence Tom Daschle’s decision (I’m sure he reads HIStalk religiously and appreciates the counsel). A new reader-suggested poll to your right asks who should follow Brailer and Kolodner in the government’s big HIT chair. Vote for one or write in your own choice since that’s what democracy is all about.
Dann, the keeper of the HIStalk Fan Club on LinkedIn, tells me that over 400 folks have signed up. I see several familiar names and faces as I scroll through the list, so hello to everybody there. LinkedIn is doing some cool things, providing a discussion forum within groups and offering tie-ins to other apps (I’ve added the HIStalk RSS to my profile so you can see story excerpts right from there). I was also trying out a cool UK-based collaboration / social networking app called Huddle when I noticed that it, too, can be connected into LinkedIn as a widget. I was thinking about doing some kind of private workspace for groups (fan club members, CIOs, sponsors – obviously I’m looking for an excuse to play around and find a problem for the Huddle solution since it looks like fun). As always, Inga and I will approve all connection requests since LinkedIn is now a competitive sport, much like getting your high school yearbook signed by the cool kids or at least bunches of the not-so-cool ones. I see some of the magazines have started their own fan clubs (losers!) but I’m pleased that HIStalk’s did it on their own (we’re kind of a self-starting crowd). Thanks to everyone involved, especially Dann.


This is cool: Josh Nesbit (that’s him above on the right), a Stanford student of international health and bioethics, sets up a telemedicine-like project for a hospital in Malawi, where Internet connectivity and even electricity is uncommon. He used a freeware SMS messaging application to connect the hospital with volunteer health workers, often poverty-stricken locals themselves, who were given prepaid cell phones to exchange information with the hospital. He’s hoping to add solar panel charging for the phones and the ability to send images. Other researchers are porting the application to the Google Android mobile platform, which would eliminate the cost of the laptop. His blog (click his name above) has specific details about the types of messages being sent and the impact on patients. Bravo.
Speaking of texting: a physician volunteer in the Congo performs a life-saving arm amputation on a 16-year-old while following text message instructions sent to him by a London colleague.
Booz Allen has declared the need for the VA to modernize it and work with DoD on common systems, according to a report uncovered by Nextgov. Interesting: Gartner looked at EMR systems and found that only those from Cerner and Epic would meet their requirements. The price tag (read carefully because you’re the one paying): $1.4 to $5.2 billion over six to 17 years.
The State of New York is requiring that new hospital clinical systems connect to the Statewide Health Information Network, meaning that Mount Sinai has to run its application to spend $34 million on Epic by that group next week.
Florida Hospital (FL, duh) will use RFID to track implantable medical devices.

Quinnipiac University researchers will study whether the use of integrated sensors in the Healthsense eNeighbor system (movement detection, door sensors, bed and toilet sensors) reduces hospitalization and improves independence.
St. Vincent Indianapolis Hospital (IN) will use per review software from startup Acesis.
Some healthcare IT folks (unnamed) met with Amazon and other vendors at Harvard Medical School this week to talk about cloud computing.
We already told you this on August 1, but Perot Systems officially announces that it will roll out VistA to two hospitals and a clinic in Jordan.
Eleven children with cancer in South Australia were overdosed on etoposide due to a computer error that first arose in January 2005 and was just now discovered. The kids are all OK.
A UK hospital cancels blood tests this week due to computer problems from the Conficker worm, which exploits a Microsoft server service vulnerability.
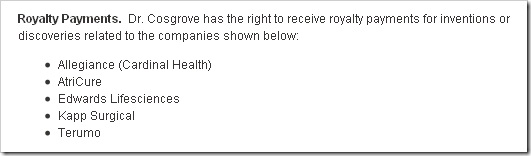
Cleveland Clinic has been panned hard in the past for its doctors (starting with its CEO) making big bucks from vendors whose products they use on patients. They aren’t saying that practice will stop, but its online physician roster will list each doctor’s financial disclosures (only companies, not amounts, but they claim they’ll add that later, maybe). The CEO’s disclosures are above. Every vendor should do what a couple of drug companies started: post every payment they make to doctors online. If it’s such an above-board practice, surely those docs won’t mind everybody knowing.
Scottish patients, including some minor celebrities, get a letter from a hospital advising them that a doctor may have inappropriately looked at their electronic medical records. The police are involved.
Detroit’s major employers are begging for handouts and threatening to take the economy down with them (much of that due to out-of-control healthcare costs), but Henry Ford’s suburban hospital — all $360 million of it — will offer walking trails and cooking lessons when finished. The CEO has zero healthcare experience, having worked at Ritz-Carlton. It’s located safely away from downtown, out where private insurance grows tall. As a hospital marketing VP I used to know always said, "We serve all, but market to few."
An interesting study: the performance of radiologists seems to improve if they’re given a photo of the patient along with the pics of their innards. They put the pictures right into the PACS.
SunTrust announces its eligibility and claims system for physician offices and hospitals.
Ohio State University’s medical school will give every student an iPod touch loaded with reference materials.
Kaiser Permanente gets a writeup for its Oakland, CA innovation center, which evaluates healthcare technology offerings from Intel, Motion, and others. The only person quoted is a doctor, but hopefully they have other kinds of professionals doing the evaluations as well.
HERtalk by Inga
I don’t know much about the world of brokering domain names, but it sounds like if you are savvy and able to secure a name before anyone else thinks it’s a great idea, the business could be profitable. HealthCareSolutions.com just sold for $55,000 and HIPAA.com went for $23,500. Curiously, www.inga.com seems to be already taken.
Glen and Trish Tullman donate $1 million to the Juvenile Diabetes Research Foundation to accelerate the development of an artificial pancreas. Their son and niece both have Type 1 diabetes. They made a similar donation to the organization in 2006.
AT&T announces plans to cut about 12,000 jobs, which represents about 4% of the company’s total workforce. Capital expenditures for 2009 will also be reduced from the 2008 levels. The company’s wireless, video, and broadband business, however, will continue to add clients to meet growing demand.
A lawsuit is filed on behalf of the Texas Faculty Association, asking that the UT System’s decision to approve massive UTMB layoffs be declared void. The lawsuit claims the decision to lay off 3,800 people violated the Texas Open Meeting Acts because the regents conducted the discussions behind closed doors. The lawsuit also questions why the UT regents purchased only $100 million worth of flood insurance and why the UT System can’t re-allocate surplus funds to prevent the layoffs.
InteGreat signs a 14-year ASP agreement with the West Virginia HealthCare Alliance to provide an EMR for its 30 network physicians.
Medical transcription provider MedQuist will pay $6.6 million to settle whistle-blower lawsuits, accused of knowingly overbilling federal clients like the VA and DOD.
Officials with the Louisiana Health Care Quality Forum claim that recent hurricanes have hampered efforts to recruit primary care physicians for a federally funded EHR demonstration project. The project has the potential to bring the state $29 million for physician practices to defray EHR costs. During the first four weeks of the application process, only 50 doctors came forward.
A survey of healthcare workers at 102 nonprofit hospitals finds that 67% of the respondents believe there is a link between disruptive physician behavior and medical mistakes. Eighteen claimed they knew of a mistake that occurred because of an obnoxious doctor. In addition, the non-profit Institute for Safe Medication Practices found that 40% of hospital staff members claimed to have been so intimidated by a doctor that they did not share their concerns about orders for medication that appeared to be incorrect. As a result, 7 percent said they contributed to a medication error.
WebMD repurchases 640,930 shares of its common stock for $12.8 million.
Sage announces its fiscal year earnings, reporting a 12% increase in revenues and a 6% increase in organic revenue growth — excluding the healthcare division, which saw an 11% revenue decline. When the healthcare’s group results were included, organic revenue growth was only 3%. On the bright side, the company says the North American management team is now in place and driving operational efficiencies.

RSNA names Gary J. Becker, MD its new president. Becker is a professor of vascular and interventional radiology at the University of AZ college of medicine.
>>> $1,600 per year? I cannot find anything that shows a capped amount.” We actually said “average,” not “maximum.”
This is all hype from CMS/Medicare. For the 2007/08 P4P project, the promised “big bucks” came out to only $600 for 40% of the physicians that were foolish enough to waste their time. A full 60% never got paid. The CMS/Medicare P4P project before that with 10 large clinics showed only 2 making a prorfit.
The e-prescribing is the same set of empty promises from CMS/Medicare. Nothing will change.
“…I released my pager and it sailed down to the bottom of the garbage pail and I never saw it again” Of course, here in (nearly) 2009 I’m sure he would say that he recycled his pager so the heavy metals contained within it wouldn’t end up in landfills and our groundwater.
For more information about the Love Settlement and the new appeal process for BCBS across the country (more or less), you can read the official documents here.
According to a few folks on the provider side, this is all a “good thing” because there is now an official, third-party review system in place where there never was before.
The problem is that the implementation, so far, differs from state to state. And the process itself is unclear. Who is this review board? Who sets the costs? Etc. NC BCBS is a good example – they still have the free appeals process they have always had, but if the insco doesn’t respond within 30 days, now, the appeal automatically goes to “Tier 2” and there is a cost. Although NC apparently has a good history of responding to appeals immediately, why would they now?
It’s interesting that you didn’t note the $310 million Henry Ford spent on its midtown Detroit city hospital. That renovation and expansion opens on Monday.
So before you cast aspersions on Henry Ford Health System for placing services near its customers, please know that we remain very committed to the city of Detroit. In the last six years we’ve opened a couple of primary care clinics here, built a multi-million dollar call center and made significant improvements to Henry Ford Hospital proper.
TPD can vouch for what Samantha is saying about Henry Ford’s commitment to improving the quality of their systems at their main facility having worked for a vendor who benefited from their purchases of high quality modality equipment.
It’s also interesting to note that the $310 million spent by Henry Ford on top of the $360 million spent in suburban Detroit is from capital ultimately generated by profits of treating patients who pay for services rendered through insurance, medicare, medicaid, self pay, etc. Unfortunately, money the auto industry is requesting as a bailout is in part due to the high cost of healthcare provided to their employees and retirees, which we all are paying for so Henry Ford can be profitable? Glad to see Henry Ford does so well in a geographic area of so much gloom… and also glad to know auto industry employees who lost their jobs can always get their healthcare at an organization who has built buildings fit for architecture and design awards. Will the Henry Ford CEO work a dollar?
“I don’t know much about the world of brokering domain names, but it sounds like if you are savvy and able to secure a name before anyone else thinks it’s a great idea, the business could be profitable. HealthCareSolutions.com just sold for $55,000 and HIPAA.com went for $23,500. Curiously, http://www.inga.com seems to be already taken.”
Although HERTalk.com is taken by a company in Taiwan, all other domain extensions are available . . .
“The e-prescribing is the same set of empty promises from CMS/Medicare. Nothing will change.”
Excuse me? Can we get back to Patient Safety as the main reason we should be moving to ePrescribing rather than $$$$. Yes, I know. But, isn’t it really just a “cost of doing business”?
Hi RustBelt:
Please quote me a study that shows that e-prescribing actually does result in “patient safety”. The closest thing I know of is one study, done at a childrens hospital that implimented a CPOE system and ended up with a higher death rate with the CPOE. Children DIED!!! Yikes!!!
I personally use Epocrates for not only drug interactions but for side effects as well as for insurance formularies. I don’t need an e-prescribing mechanism to tell me about the drugs that I write. If a sloppy, error-prone doc uses e-prescribing he still will be sloppy and error prone; the HIT won’t change that.
It is all $$$$- here we have one company (Surescripts) that has been annointed to set the industry standard which forces docs to purchase even more HIT, increasing the overall cost of doing business. It’s the patients that suffer at the end when they end up mortgaging their homes to pay off their medical bills.
Al
>>> Yes, I know. But, isn’t it really just a “cost of doing business”? <<<
Yeah- everyone seems to want for docs to pay for this cost, even though if there is a benefit, it will be for everyone but docs.
I personally can’t afford it. If you can buy it for me, then email me the cash…
Hi Al Borges,
There are studies out there through the IOM et al that demonstrate the benefits of eRx (saving lives, saving time on the phone for your office staff, etc). I won’t comment about SureScripts because that wasn’t my point. Re: the pricing…I’m not saying you need EMR (you probably don’t), I’m talking about ePrescribing only which is virtually free. Check with your Physician Organizations in your state to see if you don’t qualify. Don’t know what specialty you are, but if you do Medicare business, in a few years you will receive decreased reimbursements if you don’t have TRUE ePrescribing. Up until then, you can actually earn bonus money doing so (I know, it’s not millions but every little bit helps). I would venture to say you could get ePrescribing (standalone) for about $1-2 per day. Check it out. You might actually like it! And I would agree with you that it’s time that your health plans poney up to the table and provide incentives for this. Again, check that out, because many do right now. Good Luck!
>>> There are studies out there through the IOM et al that demonstrate the benefits of eRx (saving lives, saving time on the phone for your office staff, etc).
Rustbelt, please post a reference, and I’ll discuss it’s flaws. Most references showing increased quality, decreased errors, and cost savings are flawed in that they:
— show an inherent reporter bias
— don’t compare e-prescribing to both handwritten prescriptions and to prescriptions sent to either a fax machine or to a printer- very different things, with the latter being as legible as the typical e-prescription, but at a lower cost
— at most show that EHR with e-prescribing is associated with increased organization and better outcomes, but have not been shown to be the cause-and-effect.
E-prescribing is a workflow killer and will not be accepted by the vast majority of physicians. It’ll be one more nail in the coffin of private practice as we know it and will end up damaging Medicare by diminishing participation as physicians find themselves unable to sustain further participation in this government run program gone astray.
The biggest proponent of e-prescribing is Glen Tullman, CEO of Allscripts, who is now President Obama’s personal HIT adviser. He, his company, and his coworkers have actually donated over $160000.00 to Obama and also paid $12000.00 on 8/2008 to Daschle in “speaker fees”, all part of a massive lobbying effort that has been the underpinning of e-prescribing which is being used by those in power to pick the pockets of this nation’s physicians. It’s sleazy, unethical, but legal and bipartisan. It will do nothing to increase quality, decrease errors, or decrease costs.
Al