

Hopefully it's not through MyChart, but I've definitely heard of Secure Chat (Epic's internal messaging system within Hyperspace and Haiku)…
News 4/17/09
 From Rick Weinhaus MD: “Re: Cheezborger and usability. I agree completely. I also found Dr. Bradford’s special article in January on usability, as well as the comments, right on the mark. The promise of EHRs to improve patient care, reduce costs, and minimize errors will never be fulfilled until the software becomes more usable. As a physician, I have had first-hand experience with several EHRs. On the basis of these experiences and my sense of what mental models I actually use in taking care of patients, I have proposed two EHR design idioms to improve work flow and reduce cognitive load. If any readers would like to see detailed descriptions including graphics, they are posted as threads on the EMR Update website.” Link 1, Link 2, Link 3. Jim Bradford’s excellent article is here.
From Rick Weinhaus MD: “Re: Cheezborger and usability. I agree completely. I also found Dr. Bradford’s special article in January on usability, as well as the comments, right on the mark. The promise of EHRs to improve patient care, reduce costs, and minimize errors will never be fulfilled until the software becomes more usable. As a physician, I have had first-hand experience with several EHRs. On the basis of these experiences and my sense of what mental models I actually use in taking care of patients, I have proposed two EHR design idioms to improve work flow and reduce cognitive load. If any readers would like to see detailed descriptions including graphics, they are posted as threads on the EMR Update website.” Link 1, Link 2, Link 3. Jim Bradford’s excellent article is here.
From Pete Potamus: “Re: war game EMR predictions. How about making EMRs easier to use? This includes personalization by physician or nurse, select versus enter, dictate complex orders in ‘human’ terms; use voice recognition and personalization to present the order for review and approval. Physicians and nurses are busy people. Make it easy and they will use it. Design it so they do more work and they will resist using it. But who wouldn’t respond the same way?” I like the idea, but everybody says the same thing and the products are still never really retooled. Apple creates its own market every time it adds its considerable design expertise to otherwise pedestrian and commoditized products. Why hasn’t it happened with healthcare software? I see only two possible answers: (a) customers are buying anyway, so the redesign isn’t necessary to make sales; or (b) vendors don’t expect to get ROI from doing it even though prospects say they want it.
From Val Kelly: “Re: Epic layoffs. The last number I heard was about 400 people who were asked to resign in January and February. It’s hard to say for sure since they were told not to talk about it.”

El Camino Hospital gets a second campus and CMIO Eric Pifer gets a hospital president’s job. Interesting financial tidbits: ECH has $400 million in cash and $1.1 billion on the books (note to self: recheck the definition of “not for profit”). Not to worry though – projections are that the new place needs a daily census of only 42 patients to throw off $11 million in annual profits … sorry, margin contribution … starting the third year.
Hedge fund Tremblant Capital discloses that it has taken a 6% stake in Eclipsys.
Listening: The Cliks, an outstanding hard-rocking Canadian band (which happens to be all-LGBT). I’m desk-drumming to Oh Yeah (seventh song down in the player). And I admit I don’t watch much TV, but I’m liking 30 Rock (smart women like Tina Fey are hot, yes?) and I’m enthralled with Brit talent show singer Susan Boyle (while the cynic in me says it could be a stunt since she surely had to audition in front of someone to get there, but watching the sniggering, superficial audience and judges reduced to slack-jawed awe and near tears is still priceless). I could get pop culture if I had more time.
The son of British TV magician Paul Daniels, an IT support manager with an NHS trust, is charged with fraud for allegedly engaging a company to perform phony IT work and skimming a fee in return for approving the invoice.
JPS Health Network (TX) mulls over a potential $150 million project to implement electronic medical records, hoping to suck up some stimulus money but still worried about the upfront cost. Nobody wins those deals except Epic, so you know they’ll be calling Judy if they get their nerve up.
South Nassau Communities Hospital (NY) goes live on the Forerun ED dashboard application commercialized from BIDMC.
It’s reader survey time! It’s a quick, non-annoying way for you to let me know how to make HIStalk better for you. Here’s the link. Thank you.
A reader asked if the HIMSS presentations can be downloaded yet. They were giving a link at the conference, but the member pages don’t show the 2009 files yet.
TeraMedica will partner with Compressus Inc. to create a workflow and data management tool that will make all of an enterprise’s imaging systems and databases available from a single worklist and will support data exchange.

Natividad Medical Center (CA) hires Kirk Larson from Cerner as CIO, intriguing the local paper because he stands to make more than previous CEO ($185K and up to a 30% bonus). Seems kind of rich for a 172-bed county hospital to pay up to $240K for a CIO to run what must be a fairly small IT shop.
Two companies selling MUMPS-to-Java conversion try to convince the DoD and VA to give them a big contract to turn VistA into a semi-new system that will run on something newer than aging DEC Alphas. The estimate to develop a new system: $15 billion (!). The estimate to convert VistA to Java: $125 million over 2-5 years, including replacement servers. The problem with that kind of porting is that all the internal expertise has to start over with a new language and database (and the fact that the resulting source code is next to unreadable and free of comments to provide documentation, at least in my limited experience). And I miss the Alphas, personally.
The local health district is trying to figure out who will help Petaluma Valley Hospital (CA) pay to replace its retired A4 hospital system with Meditech. Perot told them Meditech was a logical fit, which seems kind of self-serving since it owns the former JJWILD and needs work for those people. The hospital’s parent company has Meditech and PVH can jump on for $2.8 million, but they’re worried about parting ways when the hospital lease is up.
Bad Philips numbers have investors worried about GE’s, to be reported Friday. I’m not sure how anyone could expect good GE numbers given their big exposure to bad markets (construction, manufacturing, big-ticket healthcare equipment, aviation, and of course albatross GE Capital), but maybe they will surprise positively. The stock price is at 1995 levels, but then again the Dow itself is at 1997 levels.
Backup tapes from Penisula Orthopaedic Associates (MD) containing information on 100,000 patients are stolen from a courier’s vehicle.
This is an excellent first-person story by a technologist about how bad healthcare data models nearly killed him in facilities with supposedly state-of-the-art EMRs, leading him to conclude that any kind of nationwide health network will never work. HIT people should read every word since it dashes the notion that having an EMR means improving care. “Medical personnel at urgent care and the hospital who interacted with me all used a version of the same electronic health information system (the ‘system’). It became clear that everyone was fighting that system. Indeed, they wasted between 40% and 60% of their time making the system do something useful for them … I was in ER for 20 hours before being admitted to the intensive care unit (ICU) where I spent another 28 hours. Throughout my stay, I was hooked to network attached monitors that incessantly sounded alarms to which no one responded. I was asked 11 times to repeat my medical history, medication, and allergies to as many different medical professionals. I was seen by seven doctors each of whom asked me similar questions. Five doctors were never to be seen again. All doctors mumbled something about putting their findings into the hospital’s electronic records system – most did not according to ICU nurses. No one read my allergist’s detailed report about my condition and health history.”
Groups line up against the Australian government’s plan to use patient medical records to detect Medicare fraud. "The patient record will be completely exposed, extracts obtained, copied, retained and potentially submitted in court for all to see.”
Tech Mahindra acquires Satyam for $578 million, giving it 425 acres of land, 48,000 employees, and a big footprint (not to mention a reputation sorely in need of repair, but not unsalvageable). It’s hard to believe IBM didn’t beat that bid.
Odd lawsuit: a woman microwaving hair removal wax and apparently not following instructions overheats it, then spills it as she tries to take it out of the microwave. She was burned on the thigh and chest. She’s suing the wax manufacturer for $160 million.
HERtalk by Inga
From Deborah Peel: "Re: stolen laptop at Moses Cone. The new security protections for health IT in the stimulus package require encryption of data, which will help prevent thieves from being able to use personal data in the future. But that is not enough to prevent future privacy violations like at Moses Cone. Strong state laws and medical ethics that require patient consent before medical records are disclosed were violated, but victims will have to go out and hire their own lawyers to sue hospitals and vendors to enforce these rights and protections. The stimulus package empowers state AGs to defend citizens’ privacy rights in HIPAA, but in 2002, HIPAA granted rights to hospitals like Moses Cone and over 4 million other ‘covered entities’ to disclose YOUR personal health information to outside vendors like VHA for any ‘healthcare operations’ or business use like ‘improving care’ or ‘reducing costs’ without your informed consent. Congress should have closed this giant privacy loophole in HIPAA, too."
From Large and In Charge "Re: EMR consultants. My large practice in the Midwest is looking at EHR options. Can you recommend any consultants?" If you are a consultant and/or have any names to recommend, let me know and I will forward to Large and In Charge.

The County of Los Angeles signs a contract for iMedConsent, an informed consent and patient education system by Dialog Medical. The product includes thousands of consent forms and patient education documents, plus provides digital capture of signatures and other annotations.
Allina Hospitals & Clinics settles a lawsuit with the state of Minnesota over high interest rates charged on medical debt. The not-for-profit Allina will pay patients $1.1 million to settle a dispute over whether the health system broke state law by charging patients double-digit rates on certain outstanding medical bills. Allina maintains its actions were legal.
Utah implements a new task force to stop the state’s pharmaceutical drug problem. The Utah Pharmaceutical Drug Crime Project will work to eradicate the selling, buying, stealing of prescription drugs. Utah, by the way, has the country’s highest rate of non-medical painkiller abuse. (Who’d a thunk it?)
The for-profit HCA expects its Q1 profits to much better than last year’s, in part due to higher inpatient volume and better controlled expenses. Pre-tax income is projected to be $600-$650 million for the quarter compared to $344 million last year.
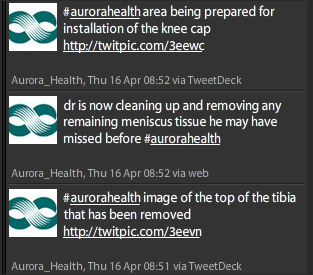
I am wondering if Twittering is going too far? Do we really need our doctors Twittering during surgery?
Regardless of the answer to that question, I am loving Twitter and have decided there are really two types of users: The Tweeterers (those who use Twitter to send out information) and Tweetees (those who primarily follow others to glean information.) I suppose there are also in-be-Tweeters who do a bit of both. I am primarily a Tweetee, though I do send out the occasional pearl of wisdom. IngaHIStalk if you want to follow.
IASIS Healthcare (TN) contracts with McKesson for the Horizon Medical Imaging PACS solution. IASIS is a 16-hospital system with approximately 2700 beds.
QuadraMed announces an agreement with e-MDs to provide QuadraMed’s hospital clients with the eMDs EHR/PM software for its affiliated physician groups. Sounds like e-MD is looking for a way to compete head-on with ECW for the hospital-supported physician EHR deals.![]()
Gateway to Care, a large FQHC system in greater Houston, selects Sevocity EHR as the system’s only funded EHR solution. Five of the organization’s health centers will implement Sevocity by August for over 200 physicians and other users.
So far this month, it looks like five new ambulatory products have achieved CCHIT 2008 certification.
I nominated Mr. H for this award, though its doubtful they would accept an anonymous blogger. But they should, don’t you think?
Mr. H should be near the top, with Inga right beside!
…oh, wait…this list was for “Most Powerful,” not Most Influential or Most Intelligent, wasn’t it? Power and influence or intelligence don’t always equate too well. If it were for the later two, Mr. H and the lovely Inga would take it going away.
Twittering from surgery is fine. Most places have a resident not involved in the surgery doing the actual typing. A lot of places are using Twitter in the med ed space.
No Epic lay offs, the number of employees continues to climb every month… I wonder, what incentive is behind the false rumors?
[From Mr. HIStalk] The person who reported this was one of those laid off. Just because the headcount is rising doesn’t mean that layoffs aren’t occurring, only that new hires are offsetting them. Great news if you’re a new hire, not so much if you’re being replaced by one.
Migrating VistA off DEC Alphas – why do they think they need to convert to Java? If VistA doesn’t run on Intersystems Cache (which I think it does), why not convert to a current Cache version, and then replace the Alphas with IBM or Sun servers as necessary…
I thought layoffs were a reduction in force. When you are eliminated from the company and a replacement is hired, isn’t that what used to be called getting fired ?
[From Mr. HIStalk] That’s a good point and a fun one for discussion! Layoffs originally meant that you were sent home unpaid for some period of time (thus the name), but would be asked to return when business picked up. Then it became a shedding of headcount overall, eliminating jobs and the people in them. For the last few years, I think most people take it to mean that companies terminate several employees as a group without documenting cause (thus differing from being being fired) but still generally acceptably meaning you might have been an underperformer who would have been asked to leave anyway, along with folks in shrinking divisions who need to cut costs. Even employees wouldn’t complain about being laid off instead of fired for cause: there’s no blot on your record, you get severance, and you leave with at least a tiny amount of dignity since you are never told directly that you weren’t making the grade. In fact, companies even use layoffs as semi-good news, announcing that “while we had an unfortunate reduction in headcount in Division X, we are actively hiring in other areas and will in fact increase total employment.” And in the rumor about Epic, it’s even more confusing because employees were supposedly not fired, but asked to resign (another non-confrontational tactic: we could fire you, but quit instead and we’ll pay your notice period and not sully your employment record as long as you agree to not say anything bad about us). Makes you wish everyone was an at-will contractor, doesn’t it?
In my experience with EMR implementations, the big reason they are unsuccessful is because as Pete Potomus says “Drs are busy people”, they want it to be flexible enough to conform to their individual standards and the customer doesn’t take ownership of the process of implementation and customization to the individual physician needs. It’s not that many of the EMRs don’t have the flexibility – it’s that the medical profession is too “busy” to take the time to learn the application, take advantage of all the functionality available and standardize their practice. Like any new “instrument” used in the practice of medicine, EMR take a lot of work to learn, tailor to the individual practice and become efficient. I’ve seen it work beautifully in a practice that takes ownership, has physician dedication to success (not just involvement) and a long term view towards incremental change. There is no “easy button” here. It takes time and work most physician feel they don’t have and don’t want to do.
I’ve worked in both the public sector and the private sector in these EMR implementations and I can tell you that it works best in the public sector because providers “must” adapt and standardize. If private sector providers don’t want to get gobbled up by the public sector in the current wave of government intervention, they better get their act together and understand that practicing the own brand of the “art” of medicine only delays and complicates the EMR implementation and adoption process.
Re: Epic
This has been going on for years. Epic thrives on overworking new college grads.
Once employees have been around for a few years, they are at the top of the pay scale, begin questioning the 60 hour weeks and traveling 3-4 wks/month, start getting married, having kids and other “distractions”. In general, it’s cleaner to threaten them with being fired or offer 2 weeks severance if they quit and replace them with a new crop of starry-eyed 20 year olds.
As an added bonus the non-compete keeps them idling for a year so they don’t use any of their knowledge to help out the struggling customers…
Regarding Rick Weinhaus’ designs and suggestions, he brings up many good points. I completely agree with both Rick and Mr. H that software has been kept in the dark ages for much too long with little, truly innovative ideas for making the user interface more usable.
On the flip side, I would caution physicians and clinicians to also think outside of the box. For those of us that were in computers in the 80’s, the first thing out of a software vendor’s mouth was ‘the system will adapt to the way you are used to doing things.’ Trying to mimick old, manual processes can also be a mistake when the technology can allow for process improvements. I’m not suggesting this is always true – there are many processes that have been around for years and are tried and true. But we do need to balance our old school thinking with the ability to capitalize on the benefits offered by the technology. At the risk of ringing a bell that has been rung many times over – analyzing workflows and capitalizing on both old and new is required.
Encryption isn’t “required” in the HITECH act, however it is strongly encouraged as it provides a “get out of jail free” card when there’s a loss of data. If it’s encrypted, loss of that information doesn’t count as a breach. In truth, encryption per se isn’t even required, it’s any ANSI-approved technology “that renders protected health information unusable, unreadable, or indecipherable to unauthorized individuals”. I don’t really know what else it could be, though, so I’m not sure why they didn’t just say “encryption”. Also, just a humorous side note, the 60 days the Secretary had to tell us what this was has come and gone already, so we’re on our own!
Also, just read the article about the lethal data model, and I can’t say that I come to the same conclusions as the author. This was at PAMF/Stanford, which as I understand it both use Epic, but as two separate installs, is that right? If so, then I would come to the opposite conclusion, that the lack of health data exchange, given a (presumably) virtually identical data model, resulted in a very frightening transition-of-care episode where the ball was dropped multiple times. Even a very basic data exchange could have prevented most of this. Not that I totally disagree with some of the comments he makes, mind you, just that his story argues the opposite of his conclusion (to me). This kind of thing happens all the time (inexcusably) in the paper record world.
The other piece he commented on that really stuck out to me was that data != knowledge. They apparently had entered a lot of data into the system, but nobody was using it, or at least using it effectively, and they clearly weren’t relying on the system to support their workflows. Sounds bad to me, but without more info it’s hard to know what’s going on there and if it was a workflow-system mismatch, or some other issues.
I am honestly surprised to see people questioning Epic on this blog. It’s funny that while Epic “lays off” (love Mr. H’s definition) their employees in very large numbers (400+) and hires in other areas…it goes relatively unnoticed or criticized? Is it because they are under the shelter of being a privately held company, have a reclusive CEO, or is it because they are just that much more awesome of a company? All I hear are the big EMR vendors are all bad and don’t understand anything about the healthcare industry, but it seems Epic isn’t considered to be lumped in with that list. How come?
I have had experience with Epic and they are no better than their competitors and even at times worse. They are growing at a ridiculously rapid pace (reminds of Cerner in the mid-90’s), under-deliver their products, and take eons to implement anything (not too mention are the most expensive vendor to boot). Sounds just like Eclipsys, Cerner, McKesson, Siemens, and GE…your typical “big vendors.” Can we at least agree that not one vendor has it right and move forward with the equal bashing of all vendors?
Bravo, Bugajski !
Much of today’s HIT seems to present what I’ve called a “mission hostile user experience.” Much work remains to be done to remediate this.
“User experience” is actually a formal term and is defined at http://www.interaction-design.org/encyclopedia/user_experience_or_ux.html
Mythoughts exactly writes:
“Like any new “instrument” used in the practice of medicine, EMR take a lot of work to learn, tailor to the individual practice and become efficient.”
However, unlike other new instruments used in the practice of medicine, Health IT is entirely unregulated, and the vendors unaccountable.
Have you ever considered that physicians’ reluctance to “alter their practices” to adhere to the IT might in fact be the best stance relative to patient safety in 2009?
Or is your faith it HIT absolute?
Mythoughts Exactly writes: “It’s not that many of the EMRs don’t have the flexibility – it’s that the medical profession is too “busy” to take the time to learn the application, take advantage of all the functionality available and standardize their practice.”
It would appear the Mythoughts Exactly may be confusing functionality and flexibility with usability. Suppose every time you had to start your car you had to put three keys in three different ignition locks. Suppose futher that although each key only fit one ignition lock, they all looked identical and you had no way of marking them. Even though this key system would be perfectly ‘functional’, it would present a significant, unnecessary cognitive load on you, the driver.
HIT vendors and users need to meet in the middle sometimes, because not every function/process lends itself well to computer automation, yet there is still value in getting information into computers because of other benefits arising once the information is there.
Folks also need to quit overhyping software and raising expectations higher than can realistically be met — especially in the area of saving time for the person having to enter the information.
I would hope all, including vendors, agree that vendors need to do more to vastly improve usability, which is key to acceptance and adoption, which in turn drives the benefits being sought in the first place.
I call bull on the Epic “layoffs”. Epic’s headcount as of a month ago was around 3300. 400 people from that would be more than 10 percent. If there was a 10 percent turnover in two months, it would be more widely known than this.
Let me ask this: If somebody isn’t performing at their job and are asked to leave, is that a one person layoff?
“Data modeling is not optional” (Data Modeling Essentials by Simsion & Witt)
Great article by Mr. Bugajski and a correct diagnosis of one of the main problems of the Healthcare Informatics industry.
I am a physician with a degree in computer sciences currently employed as Chief Medical Informatics Officer with a medium sized hospital in the USA. We are now in the process of setting up a clinical data repository (CDR) to store and present the users with laboratory results, imaging links and pharmacy orders on top of the diagnosis and procedures.
I found out repeatedly that vendors are not willing to share the database schema of their products with the excuse it is a proprietary document. Unfortunately and unbelievably so, many times this is just an excuse for a complete lack of such a schema. Even worse -the conceptual diagram, logical and physical data model is either non existent, poorly defined or kept in someone’s vault. The analogy that comes to mind is trying to build a house without a blueprint or with one that is kept in the builder’s vault.
With that being said, one has to wonder whether it is not more rational to build your own CDR, by-the-book, instead of wasting resources, buying a product and getting a low-quality product in the end. I guess it is the basic question of build vs. buy.
I strongly recommend anyone in the HIT industry to read the book I have quoted above. I have no doubt it will save millions of $, mountains of users ‘ frustrations and most probably a couple of lives.
Anon asks “Migrating VistA off DEC Alphas – why do they think they need to convert to Java? If VistA doesn’t run on Intersystems Cache (which I think it does), why not convert to a current Cache version, and then replace the Alphas with IBM or Sun servers as necessary…”
VistA runs on both Cache and GT.M, which are platform independent. Replacing the Alphas with AIX boxen would solve the first problem. The second problem, and the one that spurred this movement in the first place, is one of perception. Java is NEW! MUMPS is OLD. Ergo MUMPS must be bad. Someone has convinced the DOD that this is enough to warrant converting easy to read and maintain M into incomprehensible machine compiled Java.
I’ve seen quotes from those involved that this will also save a ton of money in the long run. Intersystems licenses aren’t free by any means, but converting to Java/Oracle as a cost saving measure? Really?
Mythoughts Exactly Says:
“It’s not that many of the EMRs don’t have the flexibility -”
No, they don’t. Not the kind of flexibility needed to provide the level of flexibility to have a doctor say “I need it to work this way” and be able to provide it that way in a timely fashion. There is only one way to provide that level of flexibility. And it’s not through a vendor app.
Alex Scarlat MD Says:
“one has to wonder whether it is not more rational to build your own CDR, by-the-book, instead of wasting resources, buying a product and getting a low-quality product in the end.”
There is another way. Don’t use a CDR. Instead, use the data stored in ancillary systems and go get them when you need it using web services. This is a new conceptual model to the CDR-centric EMR. I call it the virtual database, service-oriented architecture conceptual model. A couple of innovative organizations are using this model. It is much simpler and less costly. And the effort and money you would expend towards building and maintaining a CDR can be spent providing functionality to users.