

News 9/13/11
Top News

![]() President Obama declares this week to be National Health Information Technology Week.
President Obama declares this week to be National Health Information Technology Week.
Reader Comments
![]() From MT Hammer: “Re: All Type acquisition. As you reported earlier, MedQuist makes it official.” Sort of, anyway – the financial advisor to All Type Medical Transcription Services issues a press release about its role in the transaction. Reported here on August 25 by Hammer, who didn’t hurt ‘em.
From MT Hammer: “Re: All Type acquisition. As you reported earlier, MedQuist makes it official.” Sort of, anyway – the financial advisor to All Type Medical Transcription Services issues a press release about its role in the transaction. Reported here on August 25 by Hammer, who didn’t hurt ‘em.

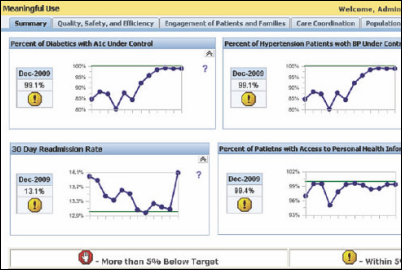
![]() From Proud athenista: “Re: athenahealth’s MU dashboards. The other day I was surprised to learn my very own company was going public with our MU transparency and just read the great interview with Jonathan Bush. Whodda thunk it would ever happen? I suggest that all vendors share their numbers.” PA is referring to last week’s HIStalk Practice interview with athenahealth CEO Jonathan Bush, who discussed the company’s decision to publish the performance of its athenaclinical clients against Meaningful Use metrics. We are happy to share similar information from other vendors, though I can only think of a couple of others that are offering those details.
From Proud athenista: “Re: athenahealth’s MU dashboards. The other day I was surprised to learn my very own company was going public with our MU transparency and just read the great interview with Jonathan Bush. Whodda thunk it would ever happen? I suggest that all vendors share their numbers.” PA is referring to last week’s HIStalk Practice interview with athenahealth CEO Jonathan Bush, who discussed the company’s decision to publish the performance of its athenaclinical clients against Meaningful Use metrics. We are happy to share similar information from other vendors, though I can only think of a couple of others that are offering those details.

![]() From Funky Bunch: “Re: Medicare attestation numbers. Here is some information from CMS that you may have seen.” CMS says $149 million has been paid as of July 31, but it doesn’t give a provider count or breakout of hospitals vs. eligible professionals. Medicaid incentive payments total $248 million and registrants for both programs total 77,549. Hospitals would get pretty big checks for their Medicare attestation, so that number might represent a fairly low number of EPs. On a related page, CMS answers the question of whether audits will be performed: maybe, so keep your documentation for at least six years, it says, else the payment “will be recouped.”
From Funky Bunch: “Re: Medicare attestation numbers. Here is some information from CMS that you may have seen.” CMS says $149 million has been paid as of July 31, but it doesn’t give a provider count or breakout of hospitals vs. eligible professionals. Medicaid incentive payments total $248 million and registrants for both programs total 77,549. Hospitals would get pretty big checks for their Medicare attestation, so that number might represent a fairly low number of EPs. On a related page, CMS answers the question of whether audits will be performed: maybe, so keep your documentation for at least six years, it says, else the payment “will be recouped.”
![]() From Just Askin’: “Re: Innovator Showcase. Is that paid promotion?” I’m kind of insulted that you would ask that, but no. Interested companies applied and my volunteer review team (investment guys and a hospital person) choose a handful from the several dozen that they felt were truly innovative based on some rather probing application questions. One of those companies happened to be a current HIStalk sponsor by coincidence and all of them earned their spot strictly on merit.
From Just Askin’: “Re: Innovator Showcase. Is that paid promotion?” I’m kind of insulted that you would ask that, but no. Interested companies applied and my volunteer review team (investment guys and a hospital person) choose a handful from the several dozen that they felt were truly innovative based on some rather probing application questions. One of those companies happened to be a current HIStalk sponsor by coincidence and all of them earned their spot strictly on merit.
![]() From Farmer Joe: “Re: Meaningful Use incentives. You seem to make a lot of implied negative statements about spending taxpayer dollars on these. Farm belt clinics are faced with closing due to low patient volume and MDs looking to retire, but with no residents who want to join them due to low pay and practices still on paper. These rural communities provide 80% of the food in this country. Every American who eats anything they don’t grow or hunt themselves should be glad to pay money to keep these practices in business to keep young farmers from quitting and moving to cities.” Sounds like a bit of a stretch that farmers will stop farming if the rest of us don’t buy EMRs for their doctors. If we have to subsidize money-losing medical practices, then I’d rather do it directly instead of paying them to adopt a particular technology that isn’t guaranteed to improve either their medical capabilities or their profitability. And I’m nearly always going to be against new government spending like HITECH, stimulus, TARP, artificial jobs creation, or whatever other cause du jour has aroused our debt-happy and votes-desperate Congress. As someone once said, “The American Republic will endure until the day Congress discovers that it can bribe the public with the public’s money.”
From Farmer Joe: “Re: Meaningful Use incentives. You seem to make a lot of implied negative statements about spending taxpayer dollars on these. Farm belt clinics are faced with closing due to low patient volume and MDs looking to retire, but with no residents who want to join them due to low pay and practices still on paper. These rural communities provide 80% of the food in this country. Every American who eats anything they don’t grow or hunt themselves should be glad to pay money to keep these practices in business to keep young farmers from quitting and moving to cities.” Sounds like a bit of a stretch that farmers will stop farming if the rest of us don’t buy EMRs for their doctors. If we have to subsidize money-losing medical practices, then I’d rather do it directly instead of paying them to adopt a particular technology that isn’t guaranteed to improve either their medical capabilities or their profitability. And I’m nearly always going to be against new government spending like HITECH, stimulus, TARP, artificial jobs creation, or whatever other cause du jour has aroused our debt-happy and votes-desperate Congress. As someone once said, “The American Republic will endure until the day Congress discovers that it can bribe the public with the public’s money.”
Acquisitions, Funding, Business, and Stock
Streamline Health reports Q2 results: a net loss of $7,000 vs. a loss of $76,000 last year; revenue $4.1 million vs. $4.7 million.
![]()
Telehealth provider Teladoc secures $18.6 million in funding
.
![]()
![]()
EDI provider MD On-Line acquires healthcare communications company Strategic EDGE Communications.
Sales

Via Christi Health (KS) purchases QuadraMed’s Identity Management solutions.

Newberry County Memorial Hospital (SC) selects Summit Healthcare to provide interface engine technology for its Meditech system.

Wilmington Health (NC) chooses Humedica MinedShare as its clinical data warehouse.
People
HHS Secretary Kathleen Sebelius announces the appointment of Leon Rodriguez as director of the Office for Civil Rights, replacing Georgina Verdugo. He was chief of staff and deputy assistant attorney general in the Justice Department’s Civil Rights Division. He was nominated by the President last December to be Administrator of the Department of Labor’s Wage and Hour Division, but that nomination was withdrawn last week.

vRad names Sandy Schmitt SVP of Strategy and Development. She was previously with Allina and VHA.

AT&T names its first CMIO, rheumatologist Geeta Nayyar MD, MBA. She was previously with Vangent.

MediClick promotes President Mike Merwarth (above) to CEO, taking over for Ron Kupferman, who remains chairman of the board.

Hon S. Pak, MD joins AirStrip Technologies as a senior advisor. He was previously CMIO for the Army Surgeon General and is an innovator in telemedicine, particularly teledermatology, and is a graduate of the United States Military Academy and a former combat medic.
Announcements and Implementations
HIMSS names four additional winners of its 2011 Davies Awards of Excellence: Kaiser Permanente (Organizational / Epic); Fallon Clinic (Ambulatory / Epic); James F. Holsinger, MD (Ambulatory / e-MDs); and Hudson River Healthcare (Community Health Organization / eClinicalWorks).
McKesson introduces McKesson Practice Choice, a Meaningful Use certified, Web-based integrated EHR/PM solution for small, independent primary care practices. The company also announces McKesson Practice Care, a service line that offers patient-centered medical home consulting in conjunction with AAFP’s TransforMed and available exclusively for practices running Practice Partner, Medisoft Clinical, Lytec MD, and Practice Choice.
Zynx Health will hire 40 new employees, including those with technical and sales experience.
Anvita Health is awarded a patent for a decision support system that can apply a variable medication patient co-pay, which it calls “dynamic, context-specific pricing.” Its intended use is to encourage optimal prescribing by charging the patient extra if he or she insists on getting prescriptions for drugs known to lack efficacy or safety. Co-pays can be reduced if a patient accepts a less-expensive cancer drug that matches responsiveness markers, or if patients are compliant with their prescribed meds.

A group of University of Alabama in Huntsville professors launches Decision Innovations, whose first product is a nurse staffing dashboard started as a 2008 pilot project with Catholic Health Initiatives. The company won the $100,000 Alabama Launchpad 2011 Business Plan competition and is setting up shop now.
Health benefits provider WellPoint signs a deal to develop commercial healthcare applications using IBM Watson technology. Few specifics were given, but the press release suggests that the applications could help physicians choose treatment options and direct patients to providers who have the best track record in treating their condition. WellPoint says it will start pilot projects early in 2012.
Government and Politics
HHS awards $8.5 million to 85 community health centers in Beacon Communities for the adoption of HIT.
HHS Secretary Kathleen Sebelius reports that 80,000 providers have applied to received Meaningful Use incentive payments and 70% of primary care physicians in rural communities have signed agreements with RECs.
A proposed HHS rule would give patients direct access to their own lab test results.
Technology
![]() Microsoft previews Windows 8 (that’s the working name, anyway). This SlashGear hands-on review shows it running on a tablet (assuming someone other than Apple is making them by the time Win 8 hits the streets). The big question for me: how well does a design that looks like it was borrowed from the iPad work on a desktop using a keyboard and mouse? Microsoft is betting the cash cow that consumers and businesses want their desktop and laptop PCs to have a radically different user interface.
Microsoft previews Windows 8 (that’s the working name, anyway). This SlashGear hands-on review shows it running on a tablet (assuming someone other than Apple is making them by the time Win 8 hits the streets). The big question for me: how well does a design that looks like it was borrowed from the iPad work on a desktop using a keyboard and mouse? Microsoft is betting the cash cow that consumers and businesses want their desktop and laptop PCs to have a radically different user interface.
![]() Software that creates natural-sounding news articles from a set of facts could write medical journal articles, the company that developed it says. They claim it can compose a unique, smooth-reading article in about one minute that even experts can’t tell wasn’t written by a human.
Software that creates natural-sounding news articles from a set of facts could write medical journal articles, the company that developed it says. They claim it can compose a unique, smooth-reading article in about one minute that even experts can’t tell wasn’t written by a human.
Other
The Canadian hospital that refused to name the nurse who breached the electronic records of 5,800 patients, citing her right to privacy, changes its mind after the province’s privacy officer declares there is no such law in a newspaper’s letter to the editor. The hospital now says it will give the nurse’s name, but only to patients who state by letter that she accessed their files.

An interesting article in the Charleston, WV newspaper covers Charleston Area Medical Center’s patient transfer center, an air traffic control-like room with a huge electronic status board showing bed status in its three hospitals.
![]() I awoke this morning realizing I had been dreaming that a network technician was working to maximize the speed of my home network. I gloated when he told me how impressed he was with the labeling of all the devices, and I was school girl giddy when he complimented me on the strength of my passwords. We then discussed the merits of various printers. I am clearly overdue for a vacation.
I awoke this morning realizing I had been dreaming that a network technician was working to maximize the speed of my home network. I gloated when he told me how impressed he was with the labeling of all the devices, and I was school girl giddy when he complimented me on the strength of my passwords. We then discussed the merits of various printers. I am clearly overdue for a vacation.
![]() A former pediatric nurse at NYU Langone Medical Center says hospital employees snooped in her medical records and, from her history and diagnosis of endometriosis, assumed she was a virgin. Her co-workers then kept trying to convince the 41-year-old woman to have sex, she says, with a neurosurgeon making references to “The 40-Year-Old Virgin” movie. She’s suing the hospital for $45 million, claiming it didn’t protect her medical records.
A former pediatric nurse at NYU Langone Medical Center says hospital employees snooped in her medical records and, from her history and diagnosis of endometriosis, assumed she was a virgin. Her co-workers then kept trying to convince the 41-year-old woman to have sex, she says, with a neurosurgeon making references to “The 40-Year-Old Virgin” movie. She’s suing the hospital for $45 million, claiming it didn’t protect her medical records.
![]() Wake Forest Baptist Medical Center (NC) fires and sues a former administrative director for “unjustified, vindictive, malicious, and gratuitous actions.” His transgression: he alerted the state that it was overpaying his employer under the terms of its health plan. The state auditor agrees, saying sloppy state contracting and oversight allowed the hospital to overbill by $1.34 million. The hospital says it was none of the former employee’s business and its contract allows it to raise prices without notifying the state.
Wake Forest Baptist Medical Center (NC) fires and sues a former administrative director for “unjustified, vindictive, malicious, and gratuitous actions.” His transgression: he alerted the state that it was overpaying his employer under the terms of its health plan. The state auditor agrees, saying sloppy state contracting and oversight allowed the hospital to overbill by $1.34 million. The hospital says it was none of the former employee’s business and its contract allows it to raise prices without notifying the state.
![]() The Wall Street Journal highlights the industry’s transition from ICD-9 to ICD-10 and mentions several of the wackier codes. One of my personal favorites: V91.07XA (burn due to water skis on fire.) athenahealth’s CTO Jeremy Delinsky correctly notes that, “You have millions of transactions flowing in the healthcare system and this is an opportunity to mess them all up.”
The Wall Street Journal highlights the industry’s transition from ICD-9 to ICD-10 and mentions several of the wackier codes. One of my personal favorites: V91.07XA (burn due to water skis on fire.) athenahealth’s CTO Jeremy Delinsky correctly notes that, “You have millions of transactions flowing in the healthcare system and this is an opportunity to mess them all up.”
![]() Even Weird News Andy finds this cringe-worthy news item from China “too weird for words.” A man bathing with live eels as part of a spa’s exfoliation treatment is startled when he looks down at his private area and sees a six-inch-long eel disappearing by the obvious method of ingress. The eel found its way to his bladder on its own, but removing it required a three-hour surgical procedure.
Even Weird News Andy finds this cringe-worthy news item from China “too weird for words.” A man bathing with live eels as part of a spa’s exfoliation treatment is startled when he looks down at his private area and sees a six-inch-long eel disappearing by the obvious method of ingress. The eel found its way to his bladder on its own, but removing it required a three-hour surgical procedure.
Sponsor Updates
- Sandhills Pediatrics (SC) receives $184,000 in ARRA incentives from its use of SRS.
- MEDSEEK announces the availability of ecoSmart Patient Precision predictive analytics technology.
- Practice Fusion forecasts that 5,000 of its eligible provider clients will receive $18,000 in Meaningful Use incentives in 2011.
- Two T-System employees, CMIO Robert Hitchcock, MD and Center for Performance Excellence Manager Janie Schumaker, RN, are elected to the board of the Emergency Department Practice Management Association.
- Aspen Advisors releases a case study on the Epic implementation of St. Anthony’s Medical Center’s (MO).
- BridgeHead Software announces the successful integration of its MediStore archive technology with three leading PACS products.
- Ben Michelson of Hayes Management Consulting discusses lessons learned from ICD-9 implementations in a guest article.
- Wolters Kluwer Health releases a ProVation MD module to support participation in the ACC National Cardiovascular Data Registry CathPCI Registry.
- Thomson Reuters introduces MarketScan Treatment Pathways to analyze medical care, outcomes, and costs.
- TeleTracking Technologies announces the availability of its RTLS to the UK healthcare market.
- Cumberland Consulting Group provides a checklist of 10 things hospitals should consider as they undergo EHR implementation.
- MidMichigan Health uses Concerro’s ShiftSelect in its retiree return-to-work program.
- The AHA Center for Healthcare Governance selects CareTech Solutions and its customer San Luis Valley Regional Medical Center as presenters for its Fall Symposium.
- The Massachusetts Department of Public Health replaces its e-Forms system with Access’s electronic forms on demand solution.
- AT&T contributes $100,000 to support a mobile health initiative to use smartphones in diabetes education.
- Elsevier / CPM Resource Center will integrate its evidence-based clinical practice guidelines and documentation solution into the McKesson EMR of Medcenter One(ND).
- Iatric Systems adds the federal government’s Blue Button capability to its PtAccess patient portal, which allows patients to download their health information as a text or PDF file.
Contacts
Mr. H, Inga, Dr. Jayne, Dr. Gregg.


























































































'Samantha Brown points out that, “Healthcare, like every other industry, gets caught up in the idolatry of the ‘innovators.’”' I…